

Cardiac output drop reflects circulatory attrition after Fontan completion: serial cardiac magnetic resonance study
- PMID: 39045076
- PMCID: PMC11195729
- DOI: 10.1093/ehjimp/qyad039
Cardiac output drop reflects circulatory attrition after Fontan completion: serial cardiac magnetic resonance study
Abstract
Aims: Cardiac magnetic resonance (CMR) imaging is a main diagnostic tool in the follow-up of Fontan patients. However, the value of serial CMR for the evaluation of Fontan attrition is unknown. The aim of this prospective study of serial CMR is to describe the analysis of time-dependent evolution of blood flow distribution, ventricular volumes, and function in patients after Fontan completion.
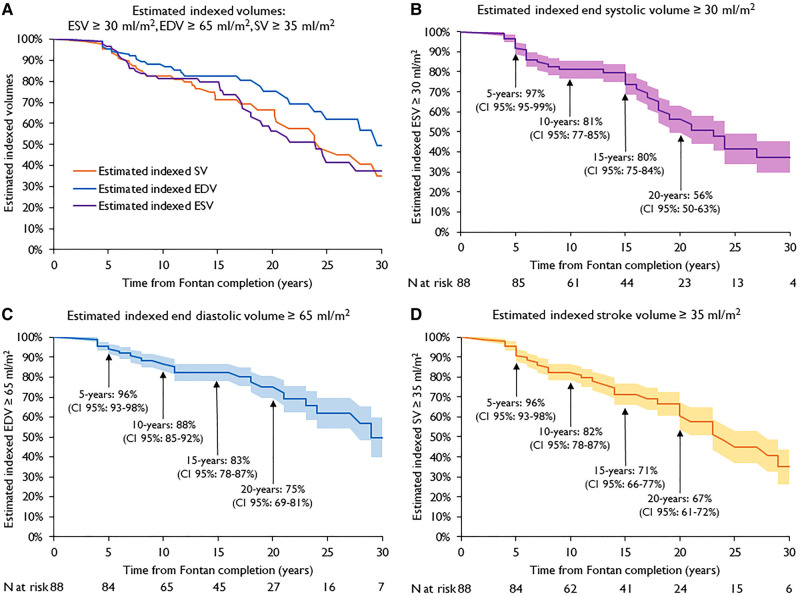
Methods and results: In this prospective single-centre study, between 2012 and 2022, 281 CMR examinations were performed in 88 Fontan patients with distribution of blood flows, measurements of ventricular volumes, and ejection fraction. Linear mixed model regression for repeated measurements was used to analyse changes of measurements across serial CMR examinations. During a time interval of 10 years, the median number of CMR per patient was 3 (range 1-5). Indexed flow of ascending aorta, caval veins, and pulmonary arteries decreased significantly across serial CMR examinations. Although a decrease of mean indexed aortic flow (3.03 ± 0.10 L/min/m2 at first CMR vs. 2.36 ± 0.14 L/min/m2 at fourth CMR, P < 0.001) was observed, ejection fraction did not decline (50 ± 1% at first CMR vs. 54 ± 2% at fourth CMR, P = 0.070). Indexed ventricular volumes did not differ significantly across serial CMR examinations.
Conclusion: The decrease of indexed aortic and cavopulmonary flows reflects the attrition of univentricular circulation and can be detected by means of serial CMR. Ventricular systolic dysfunction does not contribute significantly to this attrition. In order to detect significant change of indexed aortic flow, we recommend performing serial CMR as routine practice in the Fontan population.
Keywords: Fontan circulation; cardiac magnetic resonance; congenital heart disease; univentricular physiology.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: None declared.
Figures



References
-
- de Leval MR, Kilner P, Gewillig M, Bull C. Total cavopulmonary connection: a logical alternative to atriopulmonary connection for complex Fontan operations. Experimental studies and early clinical experience. J Thorac Cardiovasc Surg 1988;96:682–95. - PubMed
-
- Rosenthal M, Bush A, Deanfield J, Redington A. Comparison of cardiopulmonary adaptation during exercise in children after the atriopulmonary and total cavopulmonary connection Fontan procedures. Circulation 1995;91:372–8. - PubMed
-
- Rychik J, Atz AM, Celermajer DS, Deal BJ, Gatzoulis MA, Gewillig MHet al. Evaluation and management of the child and adult with Fontan circulation: a scientific statement from the American Heart Association. Circulation 2019;140:e234–84. - PubMed
-
- Ghosh RM, Whitehead KK, Harris MA, Kalb E, Chen JM, Partington SLet al. Longitudinal trends of vascular flow and growth in patients undergoing Fontan operation. Ann Thorac Surg 2023;115:1486–92. - PubMed
LinkOut - more resources
Full Text Sources