

Lateral transorbital neuroendoscopic approach for tumors of the orbital apex and spheno-orbital region: Technique, feasibility, efficacy, and safety based on a consecutive case series
- PMID: 39045588
- PMCID: PMC11263754
- DOI: 10.1016/j.bas.2024.102856
Lateral transorbital neuroendoscopic approach for tumors of the orbital apex and spheno-orbital region: Technique, feasibility, efficacy, and safety based on a consecutive case series
Abstract
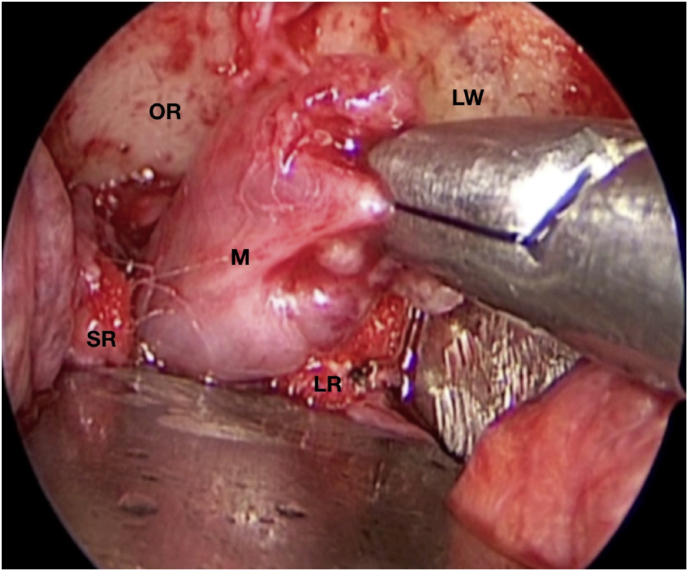
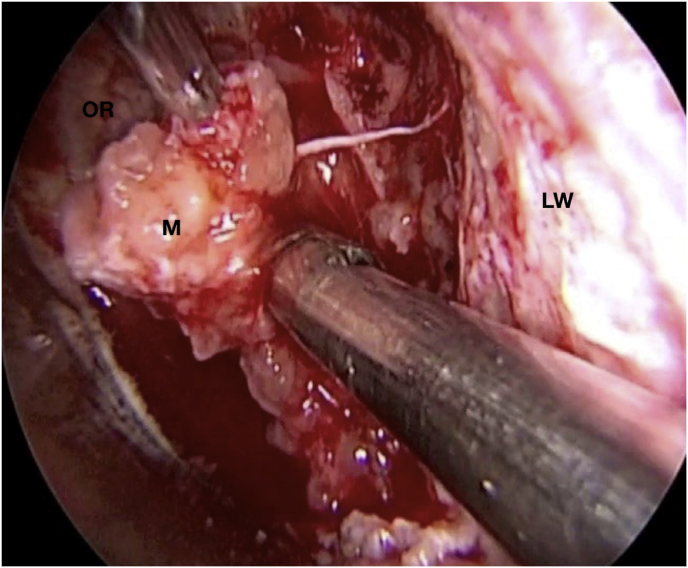
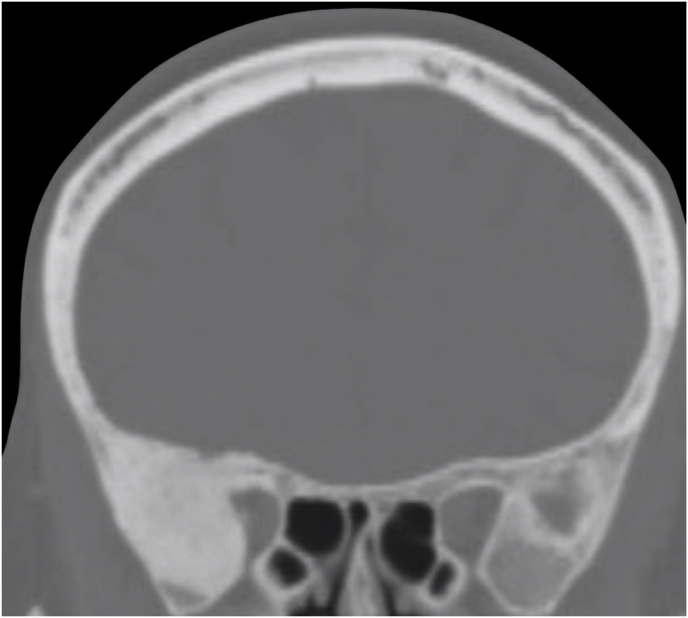
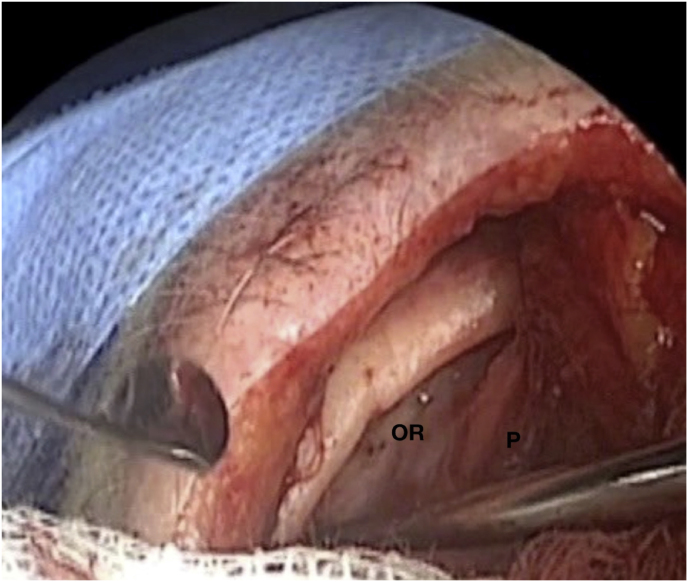
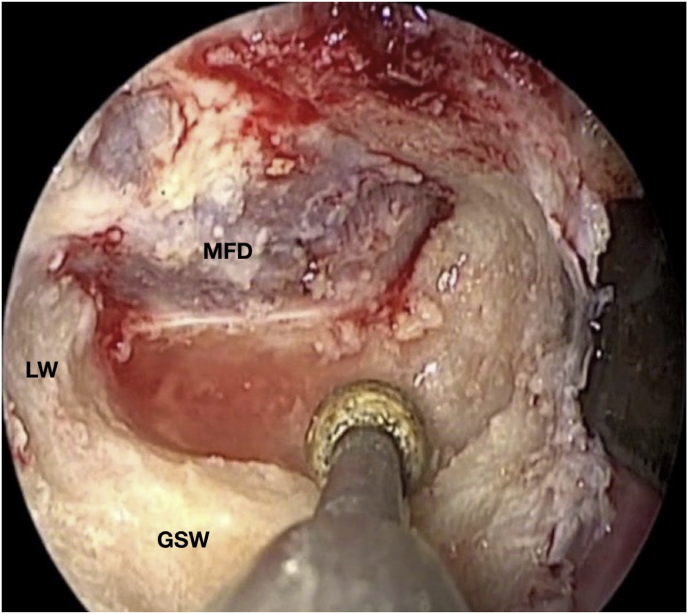
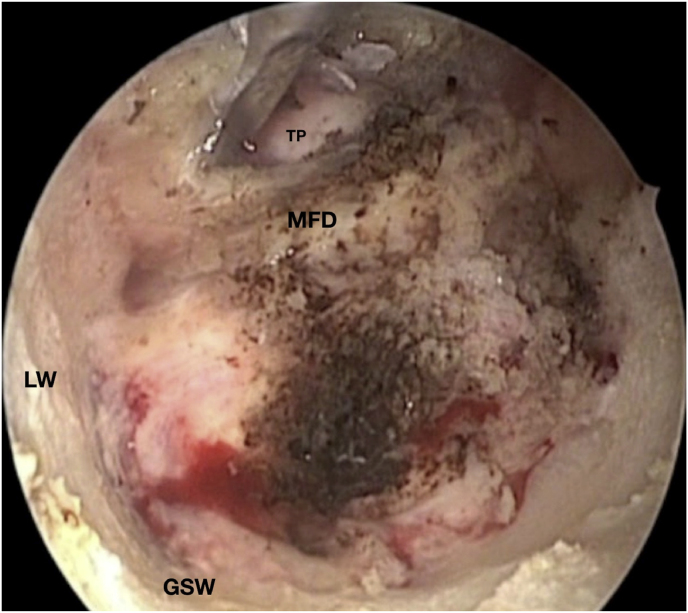
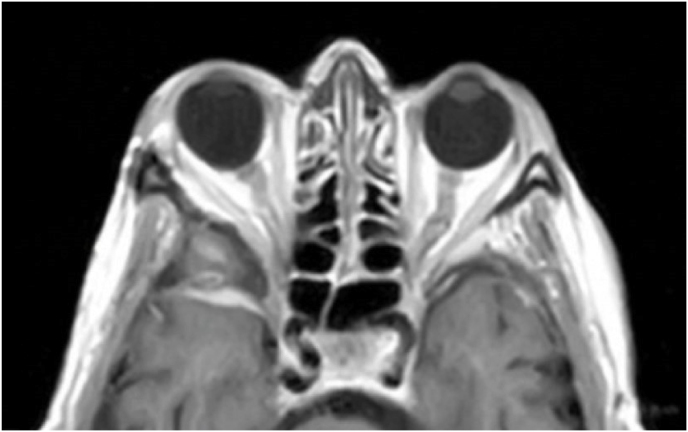
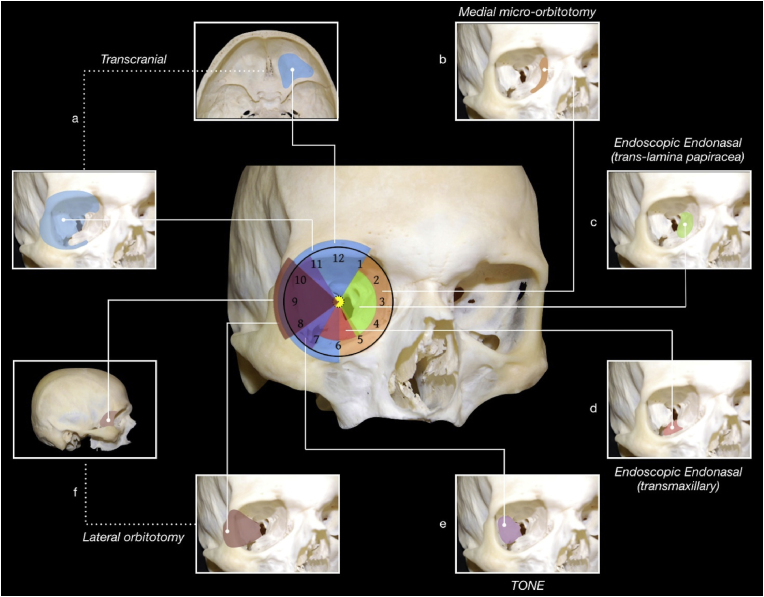
Introduction: Surgical approaches for tumors of the orbital apex and the spheno-orbital region (SOR) comprehend medial and lateral corridors. The TransOrbital NeuroEndoscopic (TONE) approach has recently been reported as a possible effective alternative to the classic lateral corridors, but literature about is still underestimated.
Research question: The aim of this study was to make a critical appraisal of the results of using the lateral TONE approach in a monocentric consecutive series of SOR tumors.
Material and methods: Data from 38 consecutive patients managed surgically by means of a lateral TONE approach for a tumor involving the orbital apex and the SOR were collected and retrospectively reviewed from 2016, January 1st to 2023, December 31st.
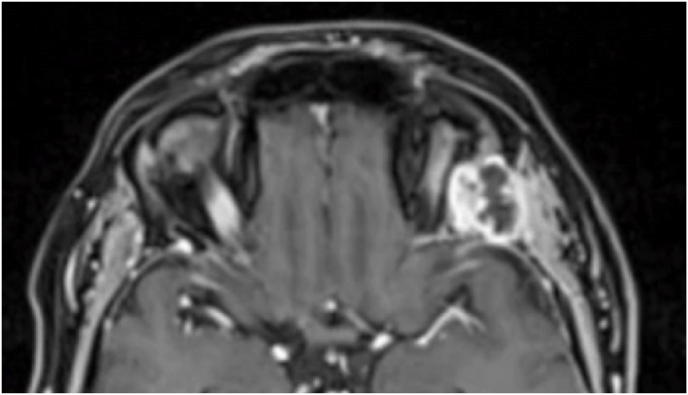
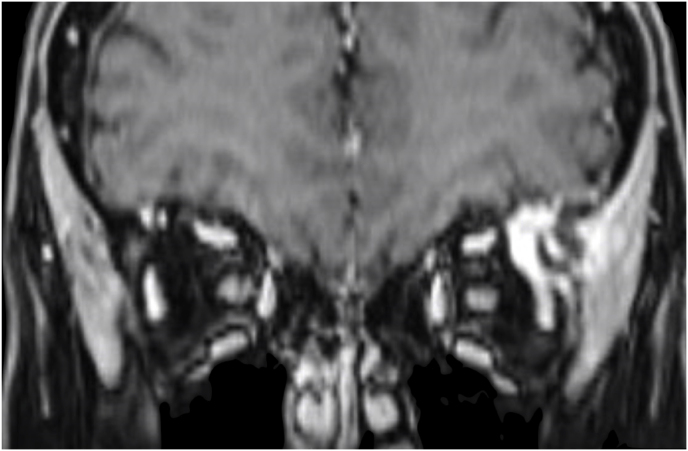
Results: Mean age was 57 ± 14,9 years (23 female). 20 tumors were intraconal, with intradural involvement of SOR in 5 cases. Gross total resection was achieved in 82,9% of the 35 cases treated with a curative intent. Average operative time was 94,8 ± 28,5 and 140,2 ± 43,3 min for extraconal and intraconal tumors, respectively. Meningiomas had an overall prevalence of 31,6%. The complication rate was 21%, of which 87,5% transient. The recurrence rate was 0 for meningiomas and 14,3% for malignant tumors based on a follow-up of 55,3 ± 26,3 and 68,6 ± 17 months, respectively.
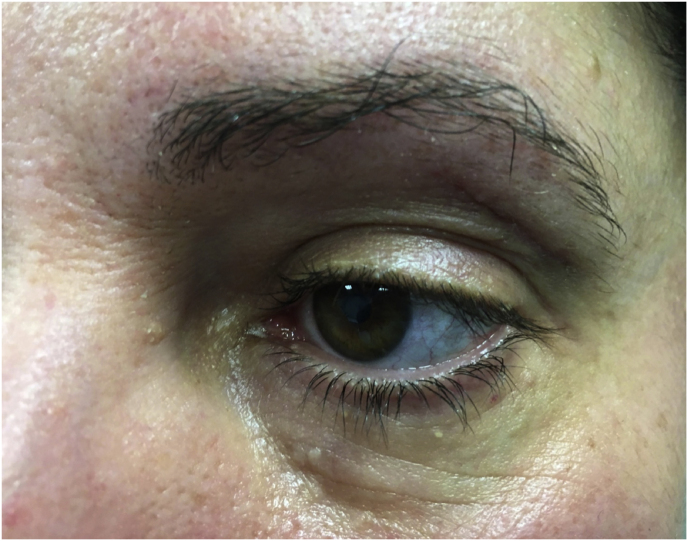
Discussion and conclusion: The lateral TONE approach is the approach of choice for tumors involving the lateral compartment of the orbital apex. It is also an effective and minimal invasive option in selected cases of spheno-orbital intradural tumors with no encasement of intracranial vessels.
Keywords: Case series; Endoscopic orbitotomy; Intraconal meningiomas; Lateral orbitotomy; Orbital approaches; Spheno-orbital meningiomas; TONE approach.
© 2024 The Authors.
Conflict of interest statement
The authors have no competing interests to declare that are relevant to the content of this article.
Figures


References
-
- Castelnuovo P., Pistochini A., Locatelli D. Different surgical approaches to the sellar region: focusing on the “two nostrils four hands technique.”. Rhinology. 2006;44(1):2–7. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
