

Concurrent epirubicin and trastuzumab use increases complete pathological response rate without additional cardiotoxicity in patients with human epidermal growth factor receptor 2-positive early breast cancer: A meta-regression analysis
- PMID: 39046067
- PMCID: PMC11267450
- DOI: 10.1002/cam4.70005
Concurrent epirubicin and trastuzumab use increases complete pathological response rate without additional cardiotoxicity in patients with human epidermal growth factor receptor 2-positive early breast cancer: A meta-regression analysis
Abstract
Background: Due to cardiotoxicity concerns, the concurrent use of epirubicin and trastuzumab has not been fully studied. This study aimed to examine the cardiotoxicity and pathological complete response (pCR) rate associated with the concurrent regimens in patients with human epidermal growth factor receptor 2 (HER2)-positive early breast cancer (EBC).
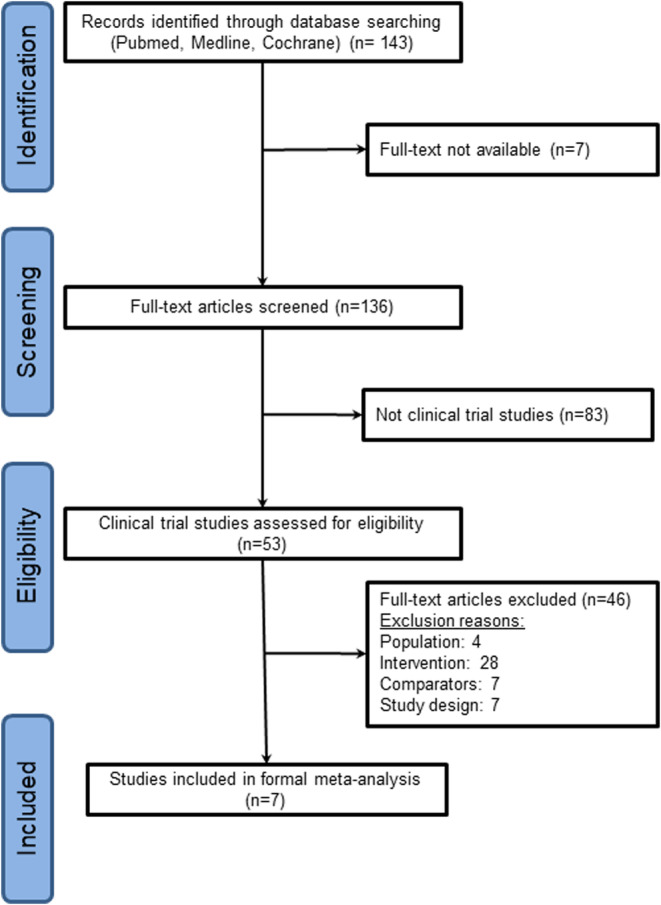
Methods: We conducted a systematic search for relevant literature in the NCBI/PubMed, the Cochrane database, and international conference abstracts for phase II or III randomized controlled trials between January 1, 2000, and February 28, 2021, focusing on the concurrent regimens in patients with HER2-positive EBC. To compare the risk of cardiotoxicity and the odds of the pCR rate, we performed linear meta-regression analyses to investigate the effects of multiple covariates.
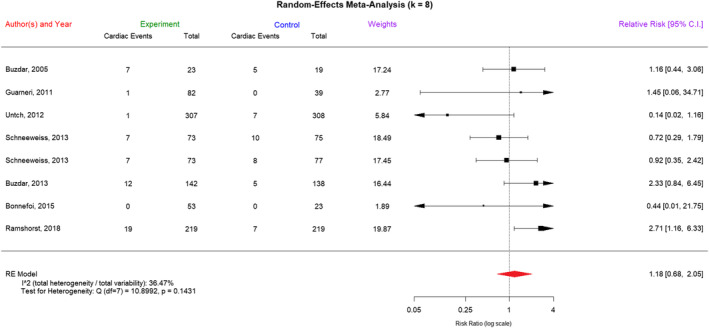
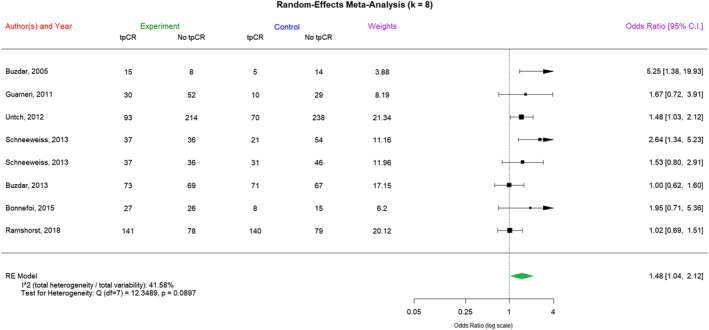
Results: We analyzed 7 neoadjuvant trials involving the concurrent use of epirubicin and trastuzumab with 1797 patients. The median cumulative dose of epirubicin used was 300 mg/m2, with a total of 96 reported adverse cardiac events. The concurrent regimens did not result in a significant increase in cardiotoxicity compared to nonconcurrent regimens (risk ratio [RR] = 1.18, 95% confidence interval [CI] = 0.68-2.05). Compared with nonconcurrent or non-anthracycline-containing regimens, concurrent regimens were associated with a significant increase in the pCR rate (odds ratio = 1.48, 95% CI = 1.04-2.12). The linear fixed-effects meta-regression analysis indicated that in trials including more patients with hormone receptor-positive EBC, the RR of cardiotoxicity significantly increased with concurrent regimens, and the pCR rate became less significant.
Conclusions: The combination of trastuzumab and a low dose of epirubicin positively impacted the pCR rate without a significant increase in cardiotoxicity. We recommend exploring concurrent regimens for HR-negative, HER2-positive tumors to enhance pCR rates, with caution advised for HR-positive tumors due to potential cardiotoxicity.
Keywords: cardiotoxicity; early breast cancer; epirubicin; human epidermal growth factor receptor 2; trastuzumab.
© 2024 The Author(s). Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
Dr. Lu reports consulting and speaker fees from Novartis, Pfizer, Roche, and Merck Sharp & Dohme and study grants from Novartis, Roche, and Merck Sharp & Dohme. The other authors have no related conflicts of interest to disclose.
Figures
References
-
- Early Breast Cancer Trialists' Collaborative Group . Polychemotherapy for early breast cancer: an overview of the randomised trials. Lancet. 1998;352(9132):930‐942. - PubMed
-
- Slamon DJ, Leyland‐Jones B, Shak S, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med. 2001;344(11):783‐792. - PubMed
-
- Vogel CL, Cobleigh MA, Tripathy D, et al. Efficacy and safety of trastuzumab as a single agent in first‐line treatment of HER2‐overexpressing metastatic breast cancer. J Clin Oncol. 2002;20(3):719‐726. - PubMed
-
- Baselga J, Carbonell X, Castañeda‐Soto N‐J, et al. Phase II study of efficacy, safety, and pharmacokinetics of trastuzumab monotherapy administered on a 3‐weekly schedule. J Clin Oncol. 2005;23(10):2162‐2171. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
