

NK- and T-cell repertoire is established early after allogeneic HSCT and is imprinted by CMV reactivation
- PMID: 39047210
- PMCID: PMC11550366
- DOI: 10.1182/bloodadvances.2024013117
NK- and T-cell repertoire is established early after allogeneic HSCT and is imprinted by CMV reactivation
Abstract
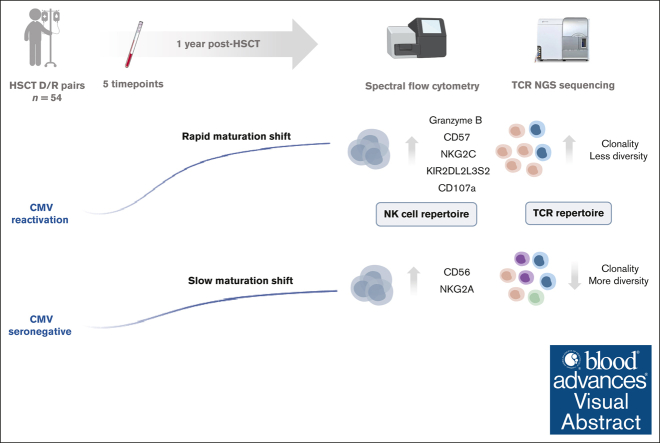
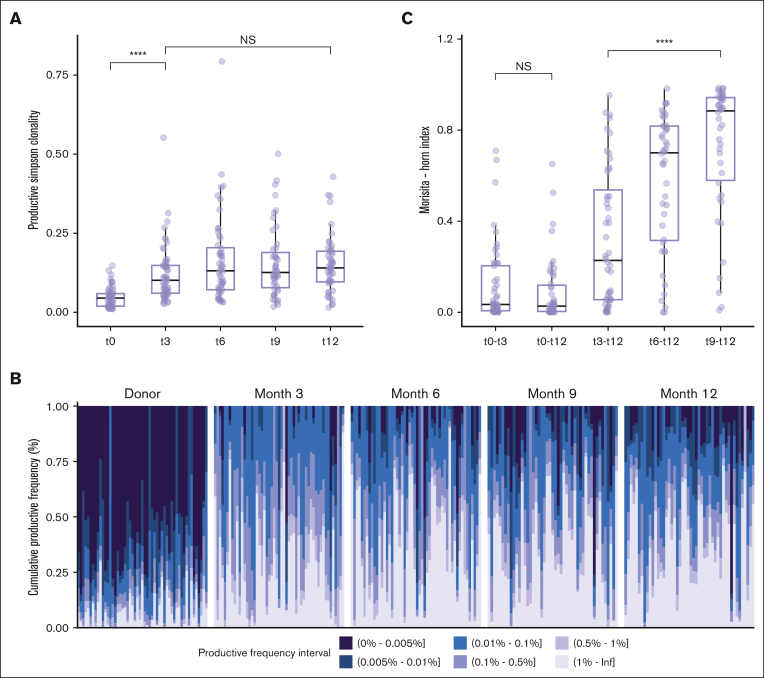
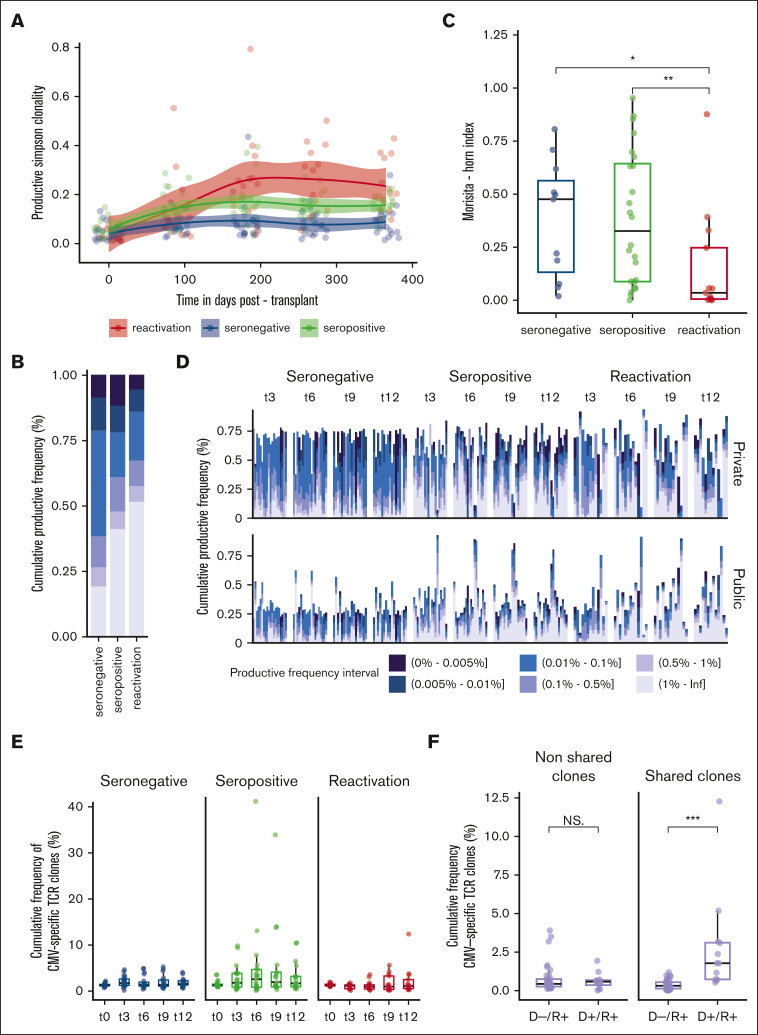
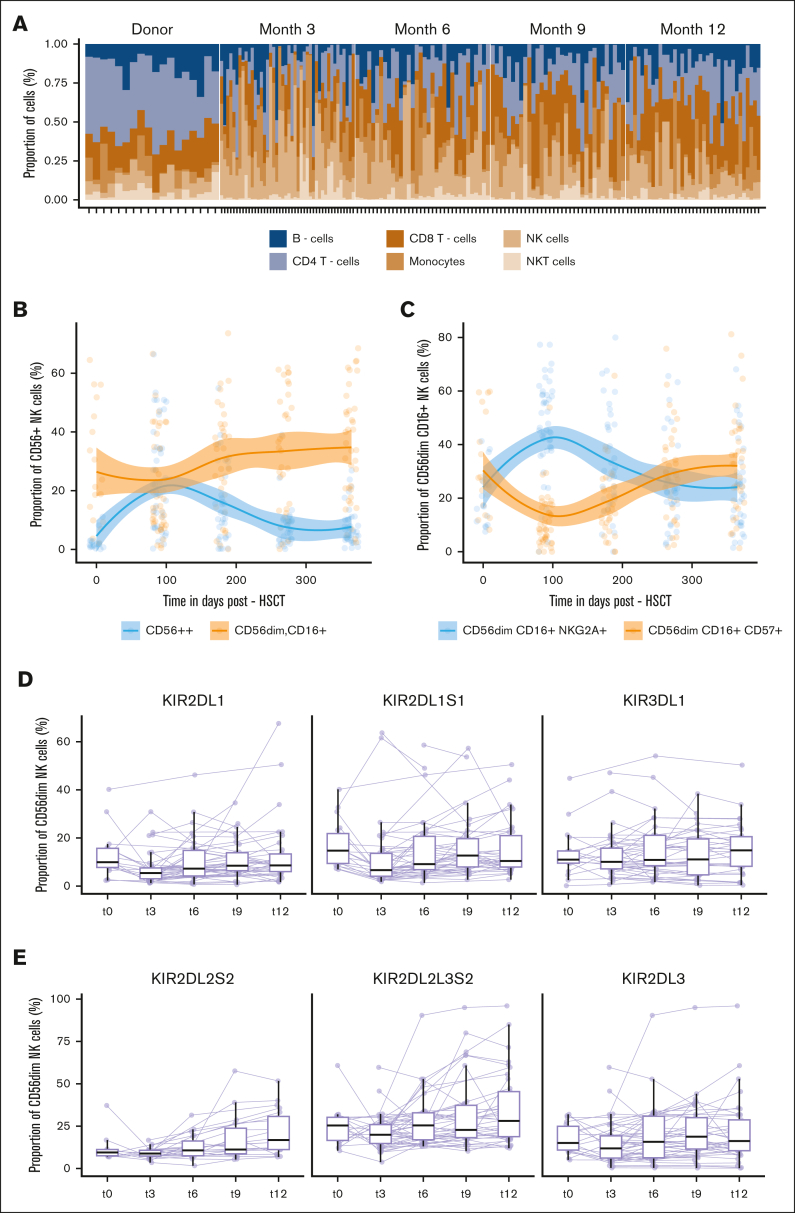
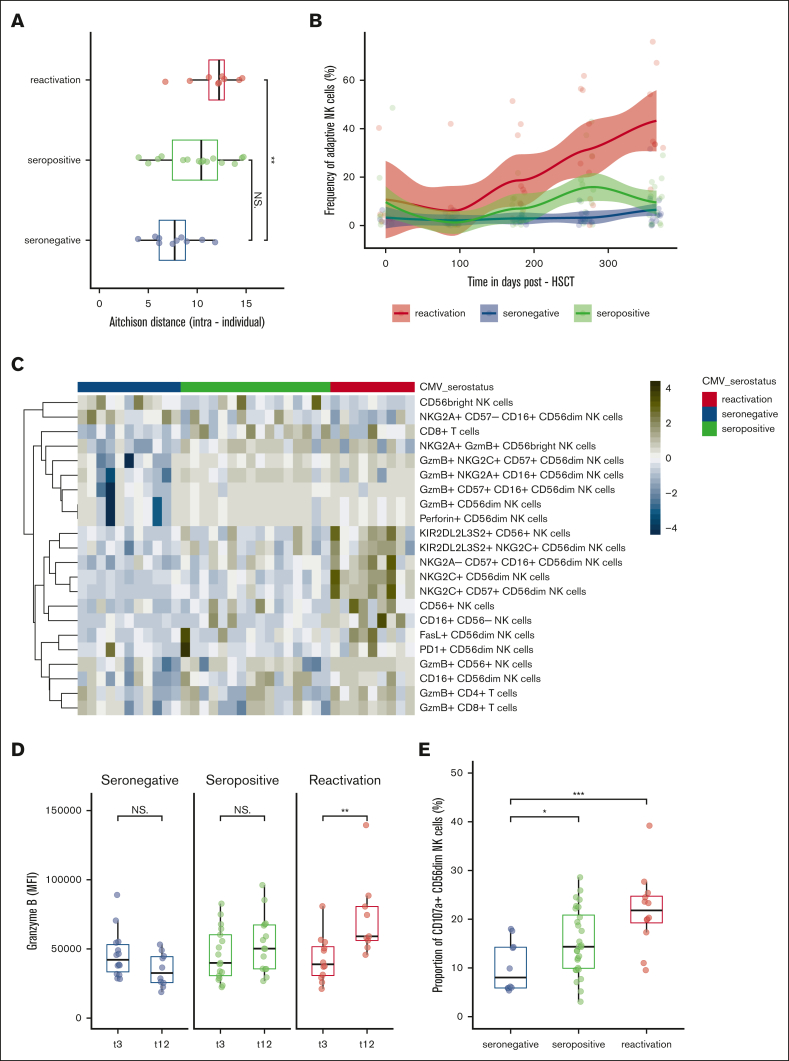
Besides genetic influences, nongenetic factors such as graft-versus-host disease and viral infections have been shown to be important shapers of the immune reconstitution and diversification processes after hematopoietic stem cell transplantation (HSCT). However, differential susceptibility to immune modulation by nongenetic factors is not fully understood. We determined to follow the reconstitution of the T-cell receptor (TCR) repertoire through immune sequencing of natural killer (NK) cells using a 35-marker spectral flow cytometry panel and in relation to clinical events. A longitudinal investigation was performed on samples derived from 54 HSCT recipients during the first year after HSCT. We confirmed a significant contraction in TCR repertoire diversity, with remarkable stability over time. Cytomegalovirus (CMV) reactivation had the ability to significantly change TCR repertoire clonality and composition, with a long-lasting imprint. Our data further revealed skewing of NK-cell reconstitution in CMV reactivated recipients, with an increased frequency of KIR2DL2L3S2+ adaptive, cytolytic, and functional CD107a+ NK cells, concomitant with a reduced pool of NKG2A+ NK cells. We provided support that CMV might act as an important driver of peripheral homeostatic proliferation of circulating specific T and NK cells, which can be viewed as a compensatory mechanism to establish a new peripheral repertoire.
© 2024 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: Y.C. reports consulting fees from Merck Sharp & Dohme (MSD), Novartis, Incyte, Bristol Myers Squibb, Pfizer, AbbVie, Roche, Jazz, Gilead, Amgen, AstraZeneca, and Servier; and travel support from MSD, Roche, Gilead, Amgen, Incyte, AbbVie, Janssen, AstraZeneca, Jazz, and Sanofi, all via the institution. The remaining authors declare no competing financial interests.
Figures
References
-
- Saccardi R, Putter H, Eikema DJ, et al. Benchmarking of survival outcomes following haematopoietic stem cell transplantation (HSCT): an update of the ongoing project of the European Society for Blood and Marrow Transplantation (EBMT) and Joint Accreditation Committee of ISCT and EBMT (JACIE) Bone Marrow Transplant. 2023;58(6):659–666. - PMC - PubMed
-
- Chabannon C, Kuball J, Bondanza A, et al. Hematopoietic stem cell transplantation in its 60s: a platform for cellular therapies. Sci Transl Med. 2018;10(436) - PubMed
-
- Storek J, Geddes M, Khan F, et al. Reconstitution of the immune system after hematopoietic stem cell transplantation in humans. Semin Immunopathol. 2008;30(4):425–437. - PubMed
-
- Buhler S, Bettens F, Dantin C, et al. Genetic T-cell receptor diversity at 1 year following allogeneic hematopoietic stem cell transplantation. Leukemia. 2020;34(5):1422–1432. - PubMed
