

Blinatumomab for MRD-Negative Acute Lymphoblastic Leukemia in Adults
- PMID: 39047240
- PMCID: PMC11334054
- DOI: 10.1056/NEJMoa2312948
Blinatumomab for MRD-Negative Acute Lymphoblastic Leukemia in Adults
Abstract
Background: Many older adults with B-cell precursor acute lymphoblastic leukemia (BCP-ALL) have a relapse despite having a measurable residual disease (MRD)-negative complete remission with combination chemotherapy. The addition of blinatumomab, a bispecific T-cell engager molecule that is approved for the treatment of relapsed, refractory, and MRD-positive BCP-ALL, may have efficacy in patients with MRD-negative remission.
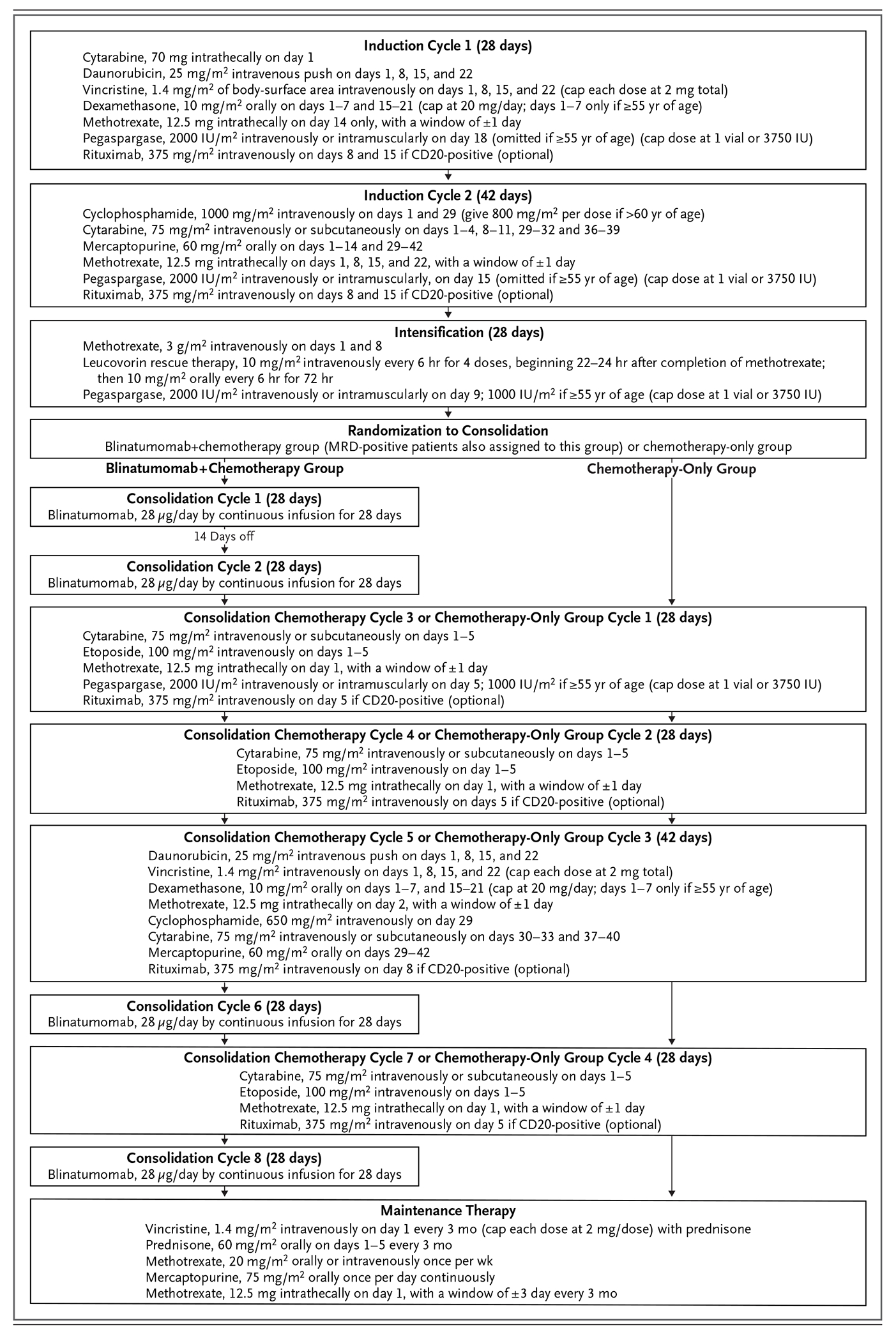
Methods: In a phase 3 trial, we randomly assigned patients 30 to 70 years of age with BCR::ABL1-negative BCP-ALL (with :: indicating fusion) who had MRD-negative remission (defined as <0.01% leukemic cells in bone marrow as assessed on flow cytometry) after induction and intensification chemotherapy to receive four cycles of blinatumomab in addition to four cycles of consolidation chemotherapy or to receive four cycles of consolidation chemotherapy alone. The primary end point was overall survival, and relapse-free survival was a secondary end point.
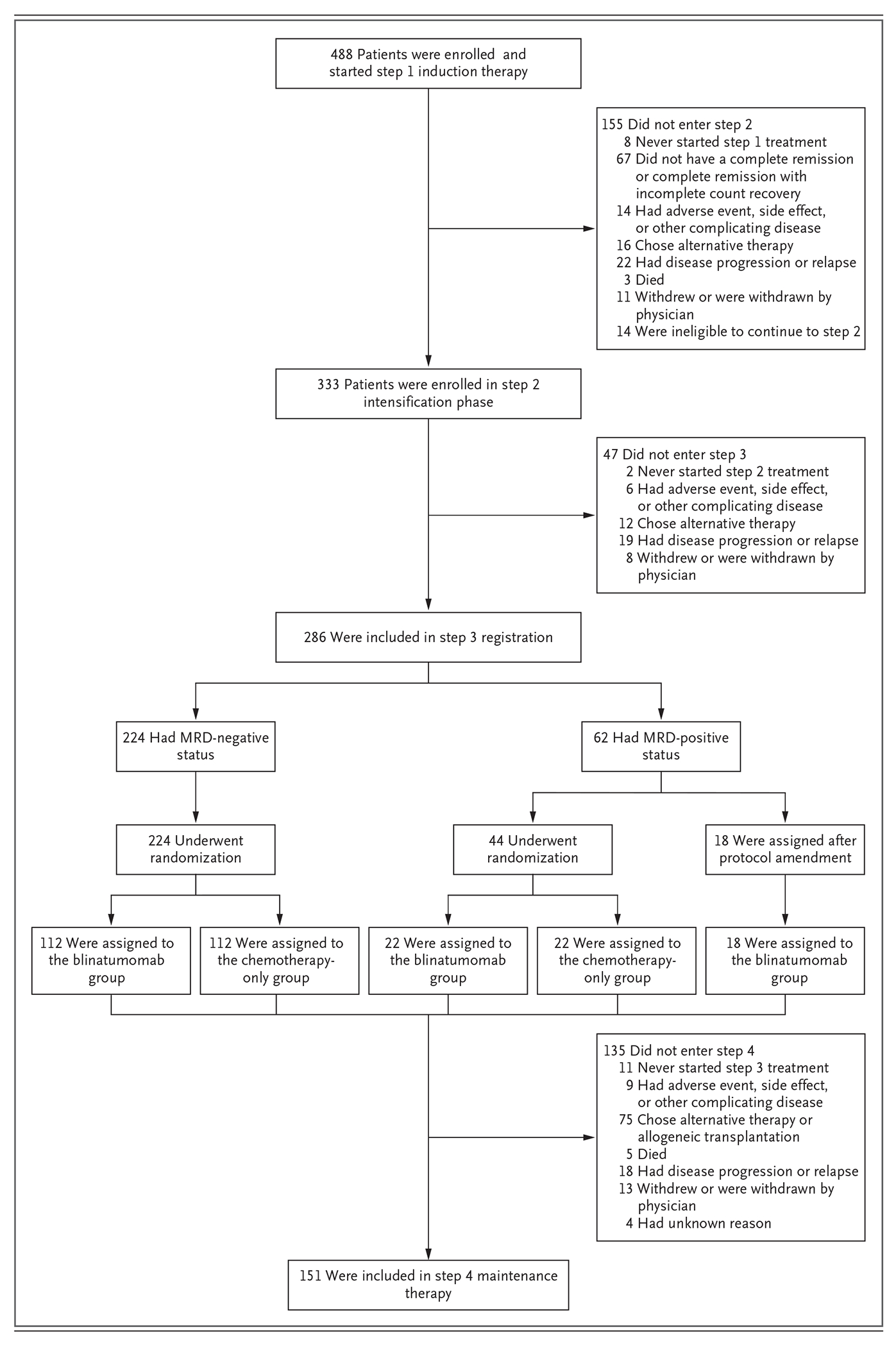
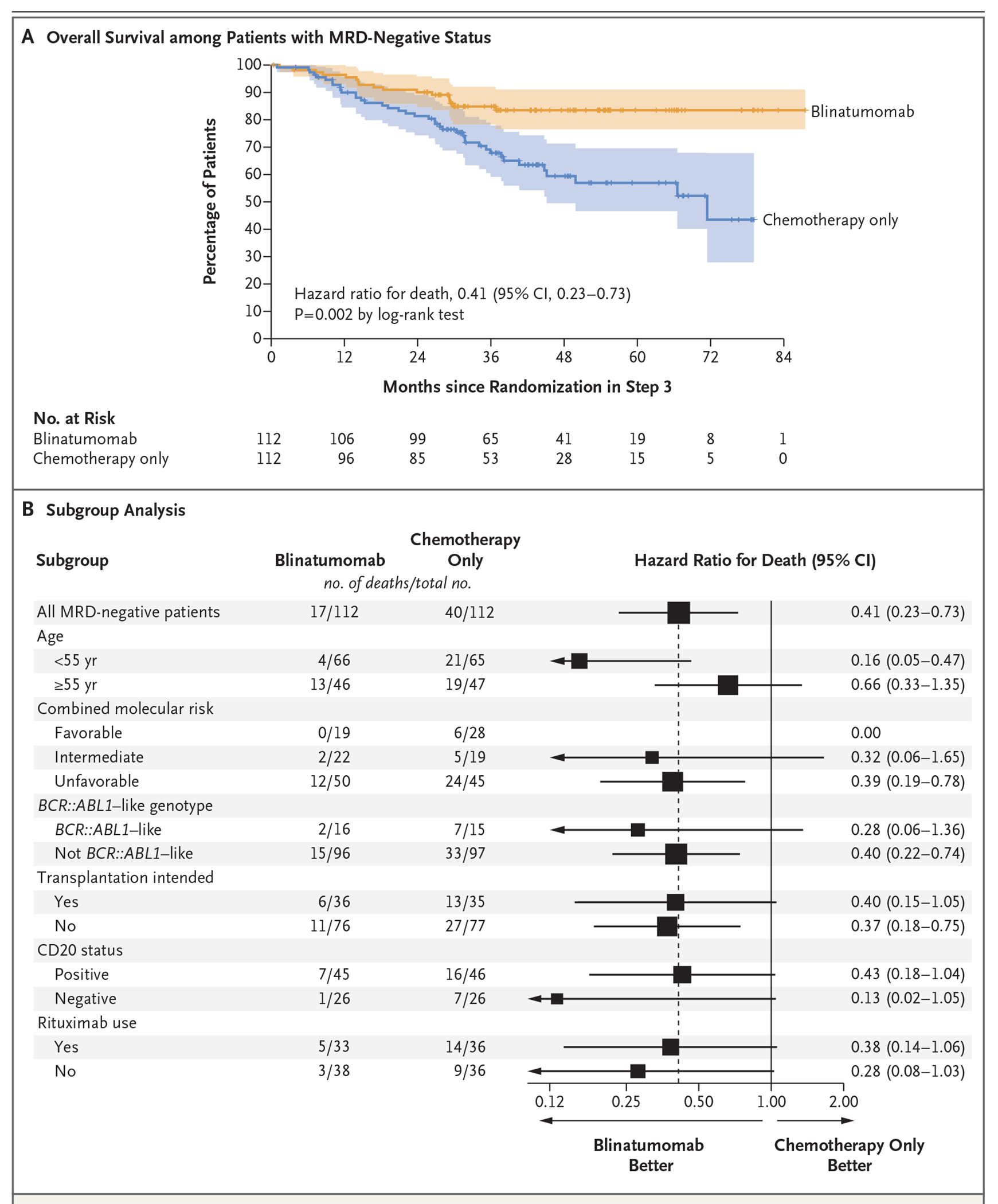
Results: The data and safety monitoring committee reviewed the results from the third efficacy interim analysis and recommended that they be reported. Complete remission with or without full count recovery was observed in 395 of 488 enrolled patients (81%). Of the 224 patients with MRD-negative status, 112 were assigned to each group. The characteristics of the patients were balanced between the groups. At a median follow-up of 43 months, an advantage was observed in the blinatumomab group as compared with the chemotherapy-only group with regard to overall survival (at 3 years: 85% vs. 68%; hazard ratio for death, 0.41; 95% confidence interval [CI], 0.23 to 0.73; P = 0.002), and the 3-year relapse-free survival was 80% with blinatumomab and 64% with chemotherapy alone (hazard ratio for relapse or death, 0.53; 95% CI, 0.32 to 0.87). A higher incidence of neuropsychiatric events was reported in the blinatumomab group than in the chemotherapy-only group.
Conclusions: The addition of blinatumomab to consolidation chemotherapy in adult patients in MRD-negative remission from BCP-ALL significantly improved overall survival. (Funded by the National Institutes of Health and others; E1910 ClinicalTrials.gov number, NCT02003222.).
Copyright © 2024 Massachusetts Medical Society.
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U10 CA180868/CA/NCI NIH HHS/United States
- UG1 CA233320/CA/NCI NIH HHS/United States
- U24 CA196172/CA/NCI NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- P30 CA021765/CA/NCI NIH HHS/United States
- R50 CA275927/CA/NCI NIH HHS/United States
- UG1 CA233198/CA/NCI NIH HHS/United States
- UG1 CA233196/CA/NCI NIH HHS/United States
- U10 CA180820/CA/NCI NIH HHS/United States
- U10 CA180794/CA/NCI NIH HHS/United States
- UG1 CA233253/CA/NCI NIH HHS/United States
- U10 CA180888/CA/NCI NIH HHS/United States
- UG1 CA233290/CA/NCI NIH HHS/United States
- UG1 CA189856/CA/NCI NIH HHS/United States
- UG1 CA233331/CA/NCI NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- UG1 CA233234/CA/NCI NIH HHS/United States
- R35 CA197695/CA/NCI NIH HHS/United States
- UG1 CA233330/CA/NCI NIH HHS/United States
- UG1 CA189859/CA/NCI NIH HHS/United States
- UG1 CA189869/CA/NCI NIH HHS/United States
- U10 CA180821/CA/NCI NIH HHS/United States
- UG1 CA233277/CA/NCI NIH HHS/United States
- UG1 CA233337/CA/NCI NIH HHS/United States
- UG1 CA232760/CA/NCI NIH HHS/United States
- U10CA180820, U10CA180794, U10CA180821, U10CA180888/ECOG-ACRIN Cancer Research Group
- UG1 CA239767/CA/NCI NIH HHS/United States
- U10 CA180863/CA/NCI NIH HHS/United States
- UG1 CA233180/CA/NCI NIH HHS/United States
- UG1 CA233339/CA/NCI NIH HHS/United States
- P50 GM115279/GM/NIGMS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous