

Mandibular movement monitor provides faster, yet accurate diagnosis for obstructive sleep apnoea: A randomised controlled study
- PMID: 39047815
- PMCID: PMC11345283
- DOI: 10.1016/j.clinme.2024.100231
Mandibular movement monitor provides faster, yet accurate diagnosis for obstructive sleep apnoea: A randomised controlled study
Abstract
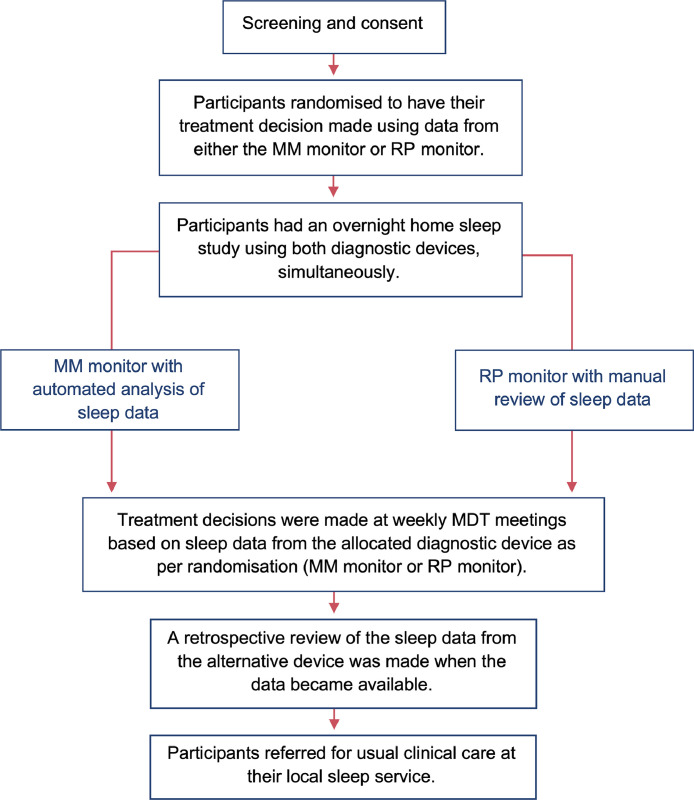
Many patients with obstructive sleep apnoea (OSA) remain undiagnosed and thus untreated, and in part this relates to delay in diagnosis. Novel diagnostic strategies may improve access to diagnosis. In a multicentre, randomised study, we evaluated time to treatment decision in patients referred for suspected OSA, comparing a mandibular movement (MM) monitor to respiratory polygraphy, the most commonly used OSA detection method in the UK. Adults with high pre-test probability OSA were recruited from both northern Scotland and London. 40 participants (70 % male, mean±SD age 46.8 ± 12.9 years, BMI 36.9 ± 7.5 kg/m2, ESS 14.9 ± 4.1) wore a MM monitor and respiratory polygraphy simultaneously overnight and were randomised (1:1) to receive their treatment decision based on results from either device. Compared to respiratory polygraphy, MM monitor reduced time to treatment decision by 6 days (median(IQR): 13.5 (7.0-21.5) vs. 19.5 (13.7-35.5) days, P = 0.017) and saved an estimated 29 min of staff time per patient.
Keywords: Diagnostic pathways; Digital health; Mandibular movement; Obstructive sleep apnoea (OSA); Remote diagnosis; Telemedicine.
Copyright © 2024 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaraton of competing interest MJM discloses being a co-applicant on a European Institute of Innovation & Technology grant, developing e-health and integrated care. MIP discloses being a paid consultant for Philips Respironics. JLK discloses speaking fees from Sunrise SA.
Figures






References
-
- Lyons MM, Bhatt NY, Pack AI, Magalang UJ. Global burden of sleep-disordered breathing and its implications. Respirology. 2020;25(7):690–702. - PubMed
-
- Guilleminault C, Eldridge FL, Tilkian A, Simmons FB, Dement WC. Sleep apnea syndrome due to upper airway obstruction: a review of 25 cases. Arch Intern Med. 1977;137(3):296–300. - PubMed
-
- Wimms AJ, Kelly JL, Turnbull CD, et al. Continuous positive airway pressure versus standard care for the treatment of people with mild obstructive sleep apnoea (MERGE): a multicentre, randomised controlled trial. Lancet Respiratory Medicine. 2020;8(4):349–358. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
