

Reduced-port robotic pancreaticoduodenectomy with optimized surgical field deployment: early results of single-site plus-two ports method
- PMID: 39048737
- PMCID: PMC11362361
- DOI: 10.1007/s00464-024-11097-y
Reduced-port robotic pancreaticoduodenectomy with optimized surgical field deployment: early results of single-site plus-two ports method
Abstract
Background: The adoption of Robotic Pancreaticoduodenectomy (RPD) is increasing globally. Meanwhile, reduced-port RPD (RPRPD) remains uncommon, requiring robot-specific techniques not possible with laparoscopy. We introduce a unique RPRPD technique optimizing surgical field exposure.
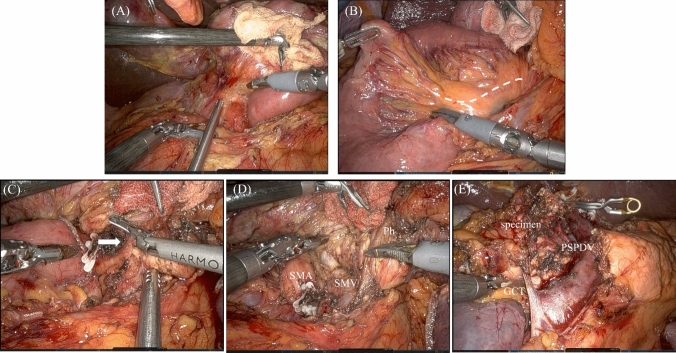
Methods: Our RPRPD utilizes a single-site plus-two ports technique, facilitated by a single-port platform through a 5-cm incision. The configuration of robotic arms (arm1, arm2, arm3, and arm4) were strategically designed for optimal procedural efficiency, with the arms2 and arm3, alongside the assistant trocar, mounted on the single-port platform, while the arms1 and arm4 were positioned laterally across the abdomen. Drainage was established via channels created at the arm1 and arm4 insertion sites. A "gooseneck traction" was principally employed with the robotic instrument to prop up the specimen rather than grasp, improving the surgical field's visibility and access. Clinical outcomes of patients who underwent RPRPD performed between August 2020 and September 2023 by a single surgeon across two centers in Taiwan and Japan were reviewed.
Results: Fifty patients underwent RPRPD using the single-site plus-two ports technique. The gooseneck traction technique enabled goodsurgical field deployment and allowed for unrestricted movement of robotic arms with no collisions with the assistant instruments. The median operative time was 351 min (250-488 min), including 271 min (219-422 min) of console time and three minutes (2-10 min) of docking time. The median estimated blood loss was 80 mL (1-872 mL). All RPRPD procedures were successfully performed without the need for conversion to open surgery. Postoperative major morbidity (i.e., Clavien-Dindo grade ≥ IIIa) was observed in 6 (12%) patients and median postoperative hospital stay was 13 days.
Conclusions: The single-site plus-two ports RPRPD with the gooseneck traction proves to be a safe, feasible option, facilitating surgical field visibility and robotic arm maneuverability.
Keywords: Minimally invasive pancreatectomy; Reduced-port robotic surgery; Robotic pancreaticoduodenectomy; Robotic surgical procedures; Single-port pancreatoduodenectomy.
© 2024. The Author(s).
Conflict of interest statement
Authors Riki Ninomiya, Masahiko Komagome, Satoru Abe, Shohei Maruta, Shinichi Matsudaira, Noriki Okada, Kazuhiro Mori, Rihito Nagata, Takehiro Chiyoda, Akifumi Kimura, Nobuyuki Takemura, Akira Maki, Yoshifumi Beck, Ching-Lung Hsieh, and Cheng-Ming Peng have no conflicts of interest or financial ties to disclose.
Figures



References
-
- Nigri GR, Rosman AS, Petrucciani N, Fancellu A, Pisano M, Zorcolo L, Ramacciato G, Melis M (2011) Metaanalysis of trials comparing minimally invasive and open distal pancreatectomies. Surg Endosc 25:1642–1651. 10.1007/s00464-010-1456-5 - PubMed
-
- Dulucq JL, Wintringer P, Mahajna A (2006) Laparoscopic pancreaticoduodenectomy for benign and malignant diseases. Surg Endosc Other Intervent Tech 20:1045–1050. 10.1007/s00464-005-0474-1 - PubMed
-
- Kendrick ML, van Hilst J, Boggi U, de Rooij T, Walsh RM, Zeh HJ, Hughes SJ, Nakamura Y, Vollmer CM, Kooby DA, Asbun HJ, Minimally Invasive Pancreatic Resection Organizing C (2017) Minimally invasive pancreatoduodenectomy. HPB (Oxford) 19:215–224. 10.1016/j.hpb.2017.01.023 - PubMed
-
- Wang M, Meng L, Cai Y, Li Y, Wang X, Zhang Z, Peng B (2016) Learning curve for laparoscopic pancreaticoduodenectomy: a CUSUM analysis. J Gastrointest Surg 20:924–935. 10.1007/s11605-016-3105-3 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
