

The complexities of decision-making associated with on-demand treatment of hereditary angioedema (HAE) attacks
- PMID: 39049074
- PMCID: PMC11271048
- DOI: 10.1186/s13223-024-00903-w
The complexities of decision-making associated with on-demand treatment of hereditary angioedema (HAE) attacks
Erratum in
-
Correction: The complexities of decision-making associated with on-demand treatment of hereditary angioedema (HAE) attacks.Allergy Asthma Clin Immunol. 2025 Apr 7;21(1):15. doi: 10.1186/s13223-025-00960-9. Allergy Asthma Clin Immunol. 2025. PMID: 40197292 Free PMC article. No abstract available.
Abstract
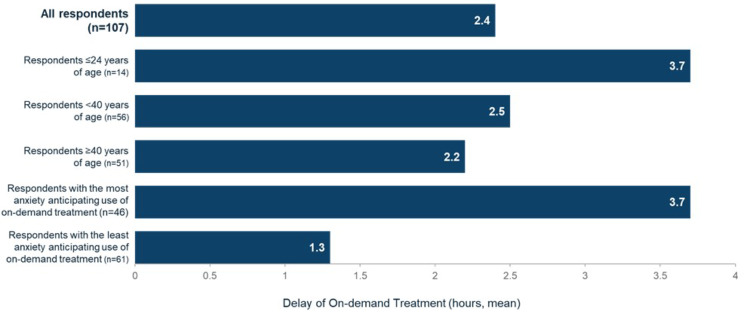
Background: Hereditary angioedema (HAE) is characterized by debilitating attacks of tissue swelling in various locations. While guidelines recommend the importance of early on-demand treatment, recent data indicate that many patients delay or do not treat their attacks.
Objective: This survey aimed to investigate patient behavior and evaluate the key factors that drive on-demand treatment decision-making, as reported by those living with HAE.
Methods: People living with HAE were recruited by the US Hereditary Angioedema Association (HAEA) to complete a 20-minute online survey between September 6, and October 19, 2022.
Results: Respondents included 107 people with HAE, 80% female, 98% adults (≥ 18 years). Attack management included on-demand therapy only (50%, n = 53) or prophylaxis with on-demand therapy (50%, n = 54). Most patients (63.6%) reported that they did not carry on-demand treatment at all times when away from home. The most common reason for not carrying on-demand treatment when away from home was 'prefer to treat at home' (72.1%). Overall, 86% of respondents reported delaying on-demand treatment, despite recognizing the initial onset of an HAE attack and despite 97% of patients agreeing that it is important to recover quickly from an HAE attack. Reasons for non-treatment or treatment delay included 'the attack is not severe enough to treat' (91.9% and 88.0%, respectively), 'cost of treatment' (31.1% and 40.2%, respectively), anxiety about refilling the prescription for on-demand treatment quickly (31.1% and 37.0%, respectively), the pain (injection or burning) associated with their on-demand treatment (18.9% and 28.3%, respectively), the lack of a suitable/private area to administer on-demand treatment (17.6% and 27.2%, respectively), lack of time to prepare on-demand treatment (16.2% and 16.3%, respectively), and a 'fear of needles' (13% and 12.2%, respectively). Survey findings from the patient perspective revealed that when on-demand treatment was delayed, 75% experienced HAE attacks that progressed in severity, and 80% reported longer attack recovery.
Conclusions: Survey results highlight that decision-making regarding on-demand treatment in HAE is more complicated than expected. The burden associated with current parenteral on-demand therapies is often the cause of treatment delay, despite acknowledgment that delays may result in progression of HAE attacks and longer time to recovery.
Keywords: Attacks; Decision-making, Burden of treatment, Survey, HAE attack journey; Hereditary angioedema (HAE); On-demand treatment.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Dreskin S. Urticaria and Angioedema. In: Goldman L, Schafer AI, editors. Cecil Medicine. 24th ed. Philadelphia, PA: Saunders Elsevier; 2011. Chapter 260.
LinkOut - more resources
Full Text Sources
Other Literature Sources
