

Impacts of three inspiratory muscle training programs on inspiratory muscles strength and endurance among intubated and mechanically ventilated patients with difficult weaning: a multicentre randomised controlled trial
- PMID: 39049092
- PMCID: PMC11271199
- DOI: 10.1186/s40560-024-00741-3
Impacts of three inspiratory muscle training programs on inspiratory muscles strength and endurance among intubated and mechanically ventilated patients with difficult weaning: a multicentre randomised controlled trial
Abstract
Background: Inspiratory muscle training (IMT) is well-established as a safe option for combating inspiratory muscles weakness in the intensive care setting. It could improve inspiratory muscle strength and decrease weaning duration but a lack of knowledge on the optimal training regimen raise to inconsistent results. We made the hypothesis that an innovative mixed intensity program for both endurance and strength improvement could be more effective. We conducted a multicentre randomised controlled parallel trial comparing the impacts of three IMT protocols (low, high, and mixed intensity) on inspiratory muscle strength and endurance among difficult-to-wean patients.
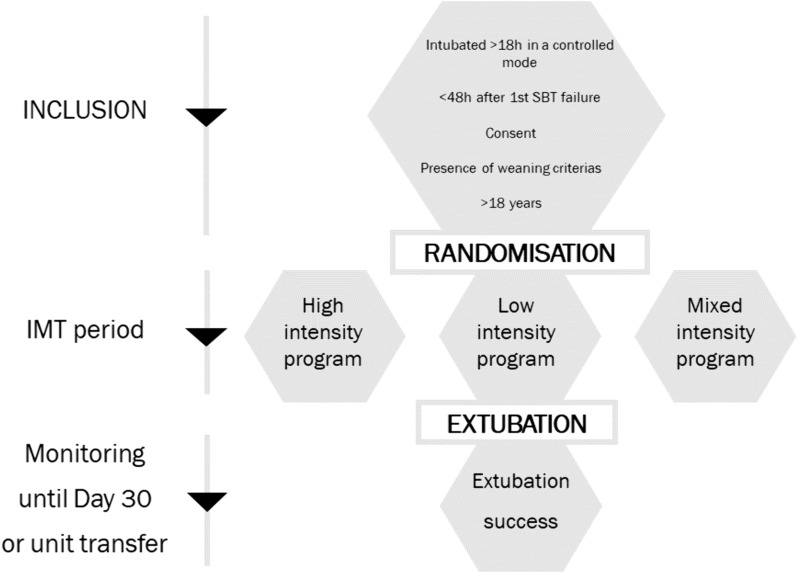
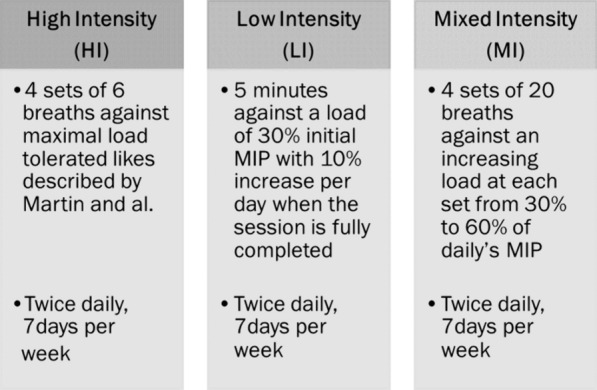
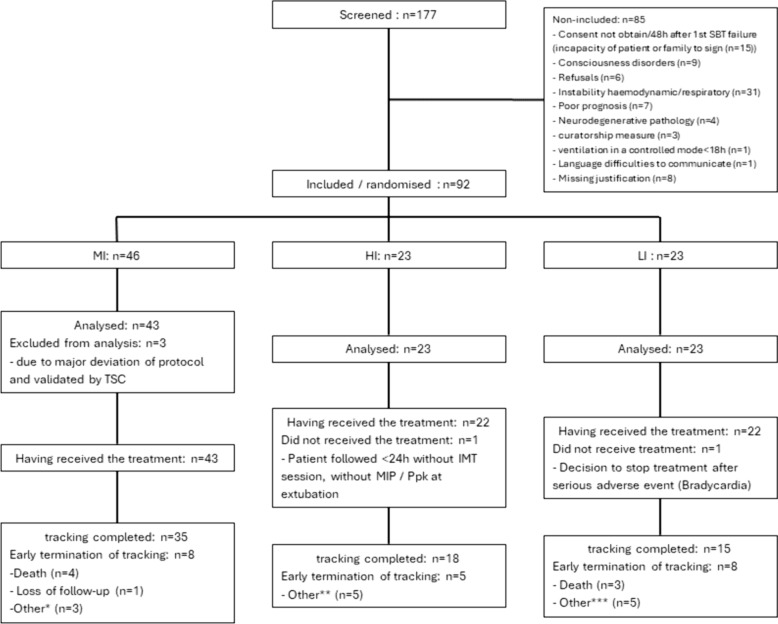
Methods: Ninety-two patients were randomly assigned to three groups with different training programs, where each performed an IMT program twice daily, 7 days per week, from inclusion until successful extubation or 30 days. The primary outcome was maximal inspiratory pressure (MIP) increase. Secondary outcomes included peak pressure (Ppk) increase as an endurance marker, mechanical ventilation (MV) duration, ICU length of stay, weaning success defined by a 2-day ventilator-free after extubation, reintubation rate and safety.
Results: MIP increases were 10.8 ± 11.9 cmH2O, 4.5 ± 14.8 cmH2O, and 6.7 ± 14.5 cmH2O for the mixed intensity (MI), low intensity (LI), and high intensity (HI) groups, respectively. There was a non-statistically difference between the MI and LI groups (mean adjusted difference: 6.59, 97.5% CI [- 14.36; 1.18], p = 0.056); there was no difference between the MI and HI groups (mean adjusted difference: - 3.52, 97.5% CI [- 11.57; 4.53], p = 0.321). No significant differences in Ppk increase were observed among the three groups. Weaning success rate observed in MI, HI and LI group were 83.7% [95% CI 69.3; 93.2], 82.6% [95% CI 61.2; 95.0] and 73.9% [95% CI 51.6; 89.8], respectively. MV duration, ICU length of stay and reintubation rate had similar values. Over 629 IMT sessions, six adverse events including four spontaneously reversible bradycardia in LI group were possibly related to the study.
Conclusions: Among difficult-to-wean patients receiving invasive MV, no statistically difference was observed in strength and endurance progression across three different IMT programs. IMT appears to be feasible in usual cares, but some serious adverse events such as bradycardia could motivate further research on the specific impact on cardiac system. Trial registration Clinicaltrials.gov identifier: NCT02855619. Registered 28 September 2014.
Keywords: Inspiratory muscle training; Mechanical ventilation; Physiotherapy; Weaning.
© 2024. The Author(s).
Conflict of interest statement
No conflict of interest related to the article exist for any of the authors involved in this study.
Figures

References
-
- Provost KA, El-Solh AA. Complications associated with mechanical ventilation. In: Tobin MJ, editor. Principles and practices of mechanical ventilation. 3rd ed. New York: McGraw-Hill Education; 2012. p. 973–94.
-
- Esteban A, Anzueto A, Frutos F, Alia I, Brochard L, Stewart TE, Benito S, Epstein SK, Apezteguía C, Nightingale P, Arroliga AC, Tobin MJ. Characteristics and outcomes in adult patients receiving mechanical ventilation: a 28-day international study. JAMA. 2002;287:345–55. 10.1001/jama.287.3.345 - DOI - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
