

Safety and effectiveness of LEO stents for dual stent-assisted embolization combined with IA and IV intra-procedural infusion of tirofiban in the treatment of wide-necked intracranial bifurcation aneurysms
- PMID: 39050127
- PMCID: PMC11268080
- DOI: 10.3389/fneur.2024.1393310
Safety and effectiveness of LEO stents for dual stent-assisted embolization combined with IA and IV intra-procedural infusion of tirofiban in the treatment of wide-necked intracranial bifurcation aneurysms
Abstract
Objective: To evaluate the safety and efficacy of employing LEO stents in dual stent-assisted embolization (DSAE) for wide-necked intracranial bifurcation aneurysms, and to assess the effectiveness of combined IA and IV intra-procedural infusion of tirofiban in mitigating perioperative complications.
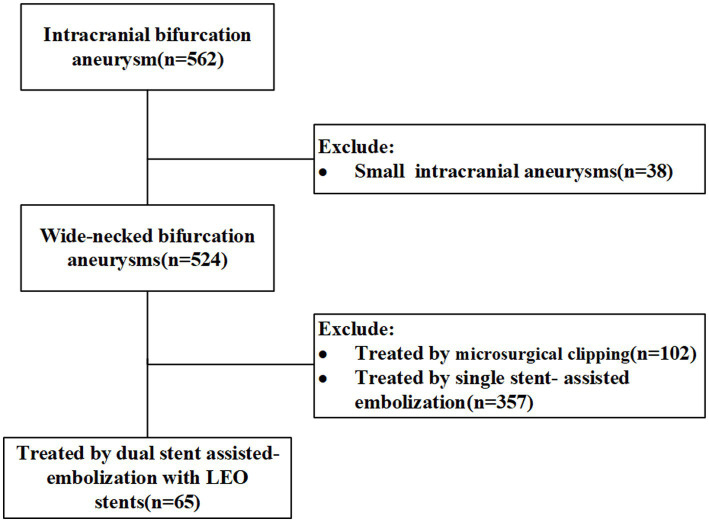
Methods: Clinical data and follow-up images from 562 patients with wide-necked intracranial bifurcation aneurysms treated at First Affiliated Hospital of Army Medical University from 2018-2022 were collected. Among them, 65 received DSAE with LEO stents. The study observed treatment success rates, procedure-related complications, perioperative thromboembolic events (TEs) and hemorrhagic events (HEs), immediate postoperative modified Raymond-Roy classification (mRR), and follow-up imaging. Glasgow Outcome Scale (GOS) at discharge and clinical follow-ups were recorded.
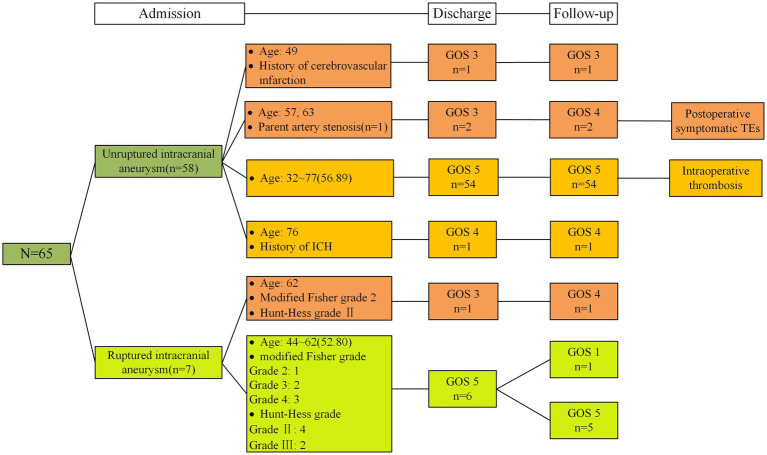
Results: The study enrolled 65 patients (mean age: 56.77 ± 10.07) with wide-necked intracranial bifurcation aneurysms. Among them, 58 had unruptured aneurysms, 7 ruptured (Hunt-Hess II-III). All aneurysms were successfully embolized without significant stent or bleeding complications. Only one case had intraoprative thrombosis; two postoperative ischemic incidents occurred within three days, no severe bleeding events. Immediate imaging showed modified Raymond-Roy classification: mRRC I (92.3%), mRRC II (4.6%), mRRC III b (3.1%). A total of 43 patients were followed up postoperatively with DSA. Among them, 41 patients exhibited mRRC I, while 2 patients exhibited mRRC II. No aneurysm was recanalized. Discharge GOS: GOS 5-60, GOS 4-1, GOS 3-4. One patient, GOS 1, died from lung cancer; others improved.
Conclusion: The utilization of LEO stents for dual stent-assisted embolization of wide-necked intracranial bifurcation aneurysms demonstrated remarkable success and safety, yielding favorable postoperative outcomes and no instances of aneurysm recurrence. The concomitant administration of perioperative antiplatelet medications alongside IA and IV intra-procedural infusion of tirofiban effectively attenuated thromboembolic events (TEs) without concomitant elevations in bleeding risks.
Keywords: antiplatelet protocol; dual stents; efficacy; safety; tirofiban; wide-necked intracranial bifurcation aneurysm.
Copyright © 2024 Wang, Lai, Zhao, Tang, Yang, Yang, Zhu and Miao.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Connolly ES, Jr, Rabinstein AA, Carhuapoma JR, Derdeyn CP, Dion J, Higashida RT, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. (2012) 43:1711–37. doi: 10.1161/STR.0b013e3182587839 - DOI - PubMed
LinkOut - more resources
Full Text Sources