

Race- and Ethnicity-Related Differences in Heart Failure With Preserved Ejection Fraction Using Natural Language Processing
- PMID: 39050815
- PMCID: PMC11268103
- DOI: 10.1016/j.jacadv.2024.101064
Race- and Ethnicity-Related Differences in Heart Failure With Preserved Ejection Fraction Using Natural Language Processing
Abstract
Background: Heart failure with preserved ejection fraction (HFpEF) is the predominant form of HF in older adults. It represents a heterogenous clinical syndrome that is less well understood across different ethnicities.
Objectives: This study aimed to compare the clinical presentation and assess the diagnostic performance of existing HFpEF diagnostic tools between ethnic groups.
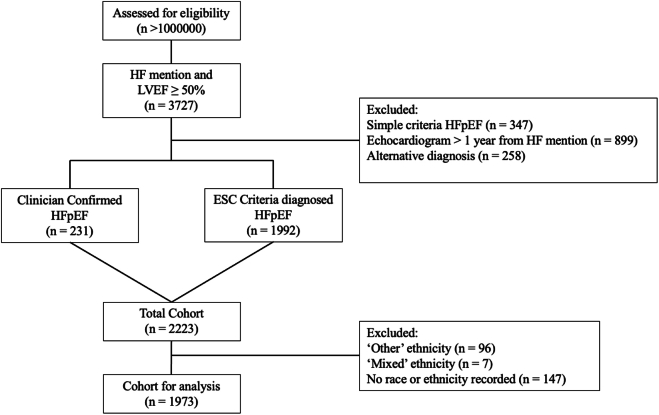
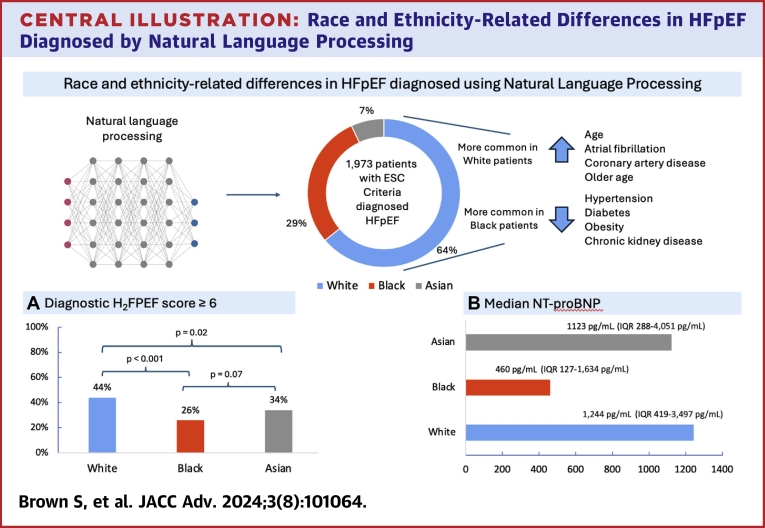
Methods: A validated Natural Language Processing (NLP) algorithm was applied to the electronic health records of a large London hospital to identify patients meeting the European Society of Cardiology criteria for a diagnosis of HFpEF. NLP extracted patient demographics (including self-reported ethnicity and socioeconomic status), comorbidities, investigation results (N-terminal pro-B-type natriuretic peptide, H2FPEF scores, and echocardiogram reports), and mortality. Analyses were stratified by ethnicity and adjusted for socioeconomic status.
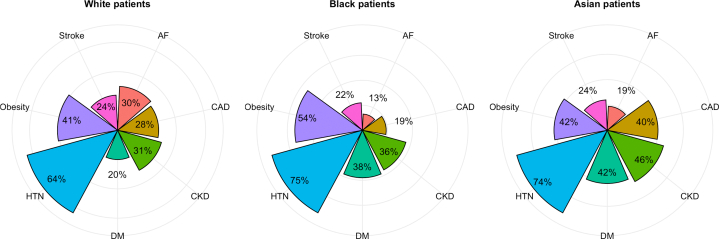
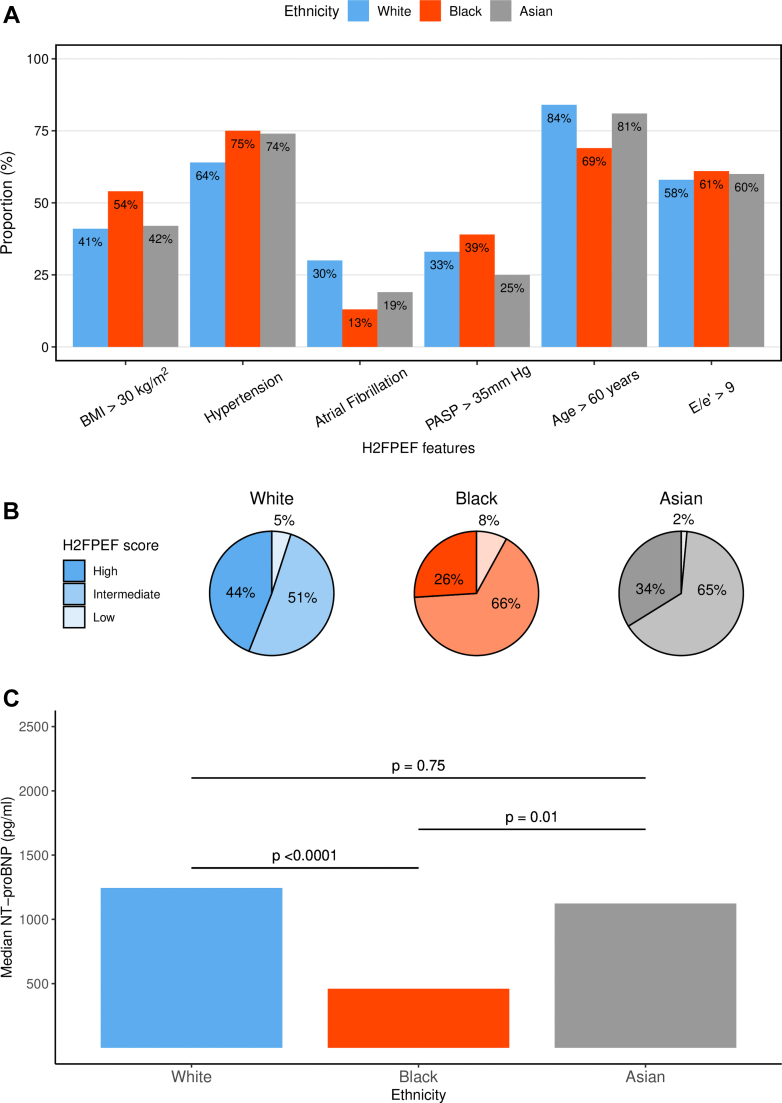
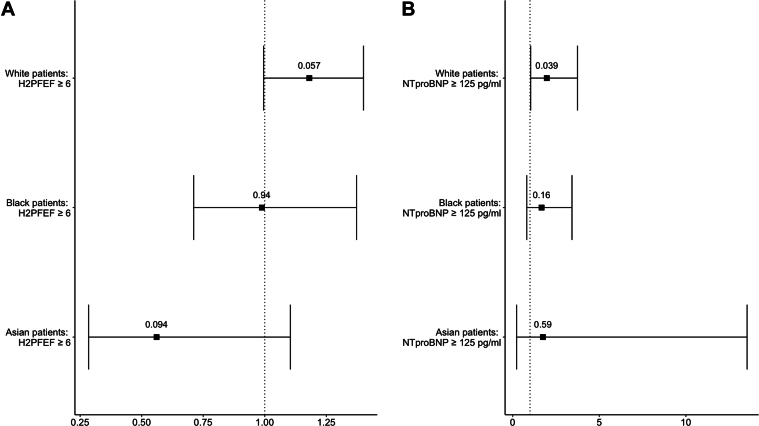
Results: Our cohort consisted of 1,261 (64%) White, 578 (29%) Black, and 134 (7%) Asian patients meeting the European Society of Cardiology HFpEF diagnostic criteria. Compared to White patients, Black patients were younger at diagnosis and more likely to have metabolic comorbidities (obesity, diabetes, and hypertension) but less likely to have atrial fibrillation (30% vs 13%; P < 0.001). Black patients had lower N-terminal pro-B-type natriuretic peptide levels and a lower frequency of H2FPEF scores ≥6, indicative of likely HFpEF (26% vs 44%; P < 0.0001).
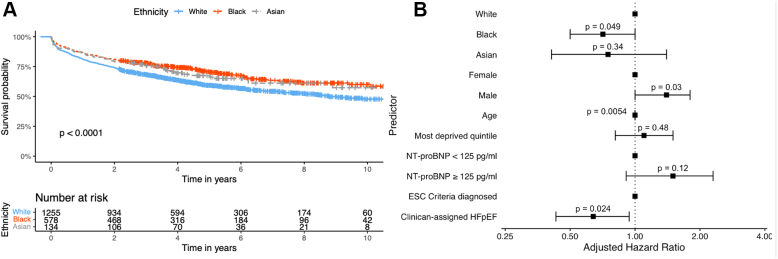
Conclusions: Leveraging an NLP-based artificial intelligence approach to quantify health inequities in HFpEF diagnosis, we discovered that established markers systematically underdiagnose HFpEF in Black patients, possibly due to differences in the underlying comorbidity patterns. Clinicians should be aware of these limitations and its implications for treatment and trial recruitment.
Keywords: AI (artificial intelligence); Natural Language Processing; health equity; heart failure; preserved ejection fraction.
© 2024 The Authors.
Conflict of interest statement
Professor Shah has served as an advisor to Forcefield Therapeutics and CYTE–Global Network for Clinical Research. Professor McDonagh has received speaker fees or advisory board fees from Abbott, Edwards, Boehringer Ingelheim, and AstraZeneca. This work was supported by grants from the 10.13039/501100000274British Heart Foundation (CH/1999001/11735, RG/20/3/34823, and RE/18/2/34213 to Professor Shah; CC/22/250022 to Dr Dobson, Professor Shah, Dr Teo, and Dr Gallagher) and King’s College Hospital Charity (D3003/122022/Shah/1188 to Dr Shah). Dr Gallagher and Dr Bromage are each supported by MRC Clinician Scientist Fellowships (MR/Y001311/1 to Dr Gallagher, MR/X001881/1 to Dr Bromage). All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures

References
-
- Borlaug B.A., Sharma K., Shah S.J., Ho J.E. Heart failure with preserved ejection fraction. J Am Coll Cardiol. 2023;81(18):1810–1834. - PubMed
-
- Owan T.E., Hodge D.O., Herges R.M., Jacobsen S.J., Roger V.L., Redfield M.M. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355(3):251–259. - PubMed
-
- Sueta D., Yamamoto E., Nishihara T., et al. H2FPEF score as a prognostic value in HFpEF patients. Am J Hypertens. 2019;32(11):1082–1090. - PubMed
-
- Verbrugge F.H., Reddy Y.N.V., Sorimachi H., Omote K., Carter R.E., Borlaug B.A. Diagnostic scores predict morbidity and mortality in patients hospitalized for heart failure with preserved ejection fraction. Eur J Heart Fail. 2021;23(6):954–963. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
