

Identifying the Mechanisms of a Peripherally Limited Exercise Phenotype in Patients With Heart Failure With Preserved Ejection Fraction
- PMID: 39051098
- PMCID: PMC11335445
- DOI: 10.1161/CIRCHEARTFAILURE.123.011693
Identifying the Mechanisms of a Peripherally Limited Exercise Phenotype in Patients With Heart Failure With Preserved Ejection Fraction
Abstract
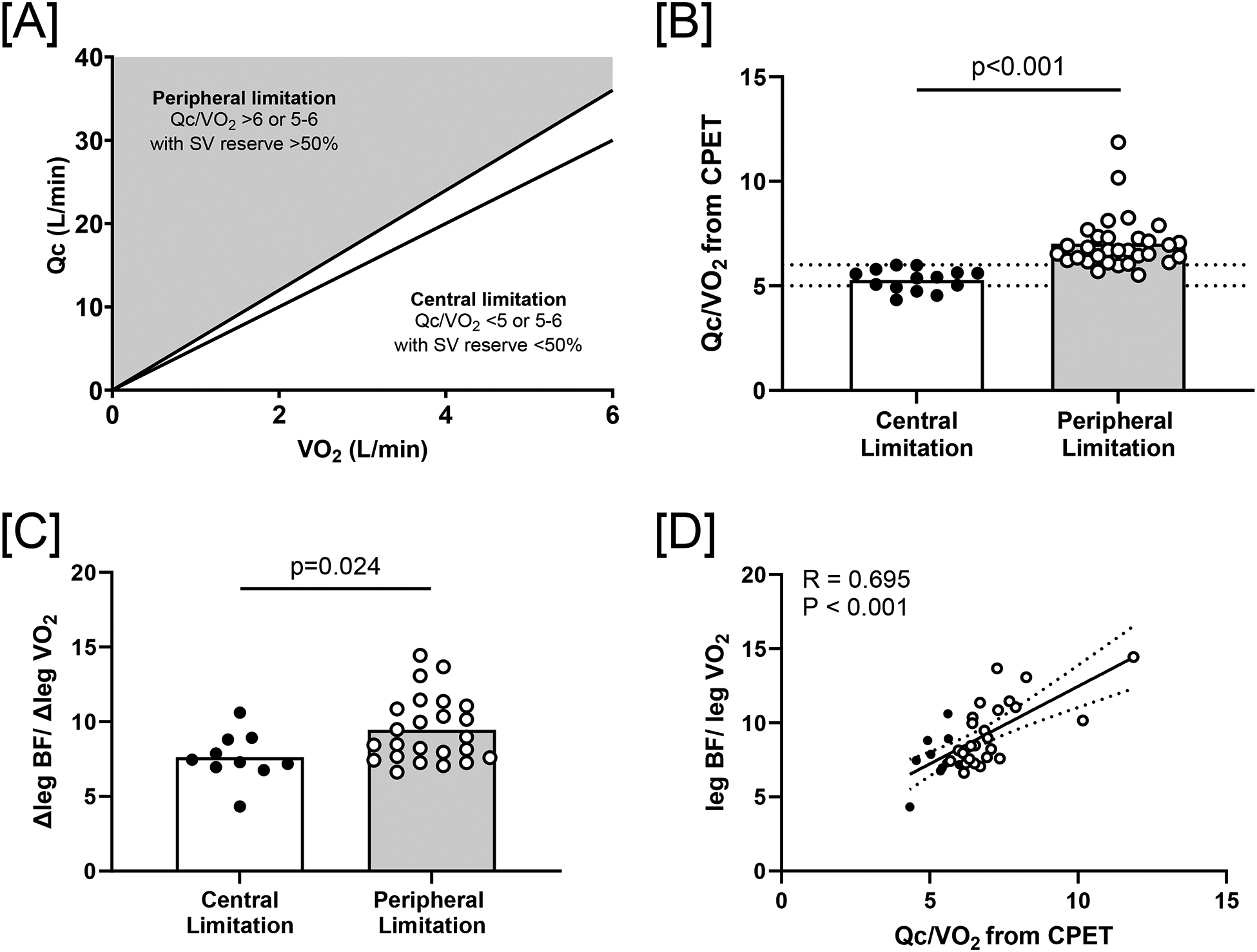
Background: We identified peripherally limited patients using cardiopulmonary exercise testing and measured skeletal muscle oxygen transport and utilization during invasive single leg exercise testing to identify the mechanisms of the peripheral limitation.
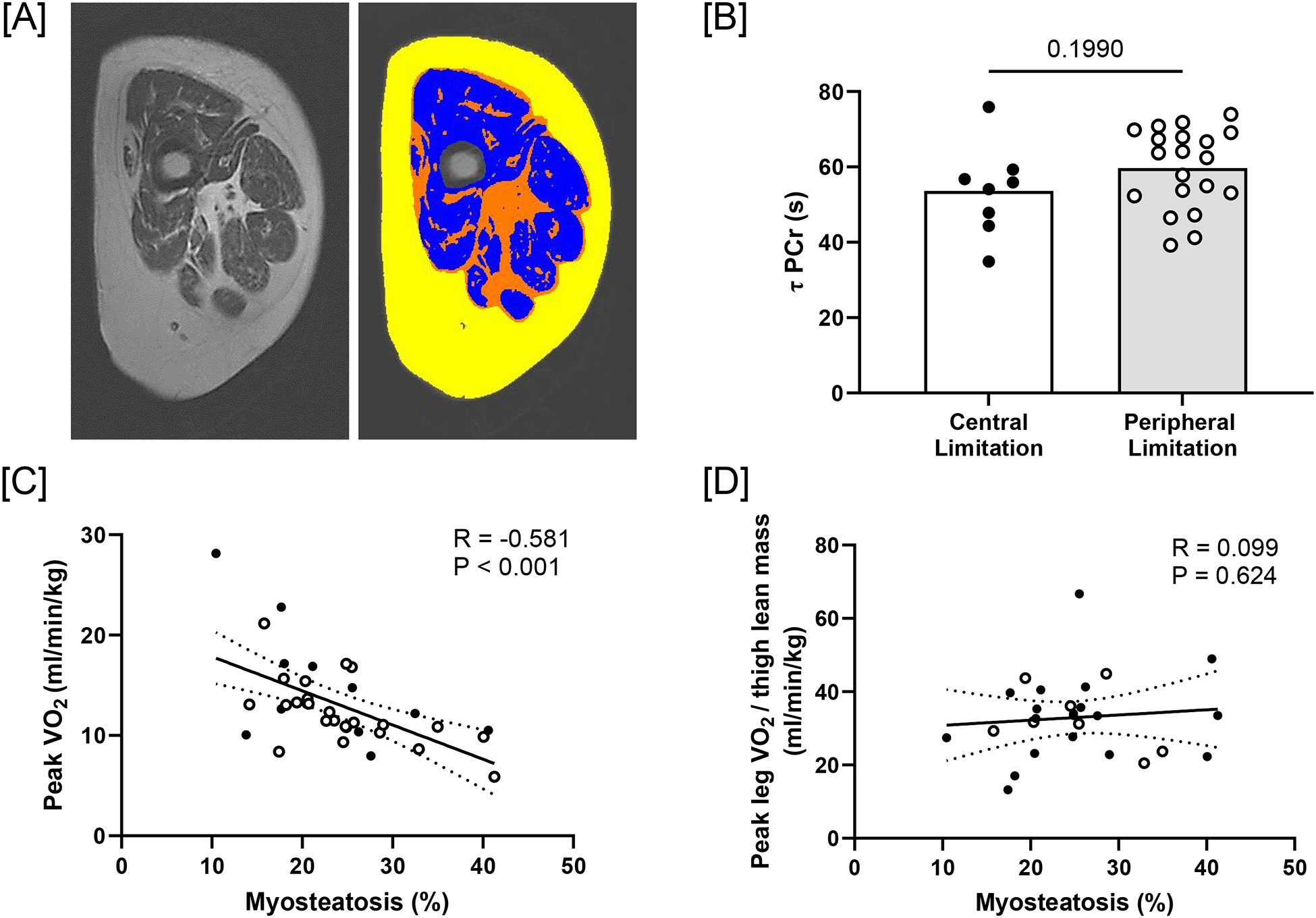
Methods: Forty-five patients with heart failure with preserved ejection fraction (70±7 years, 27 females) completed seated upright cardiopulmonary exercise testing and were defined as having a (1) peripheral limitation to exercise if cardiac output/oxygen consumption (VO2) was elevated (≥6) or 5 to 6 with a stroke volume reserve >50% (n=31) or (2) a central limitation to exercise if cardiac output/VO2 slope was ≤5 or 5 to 6 with stroke volume reserve <50% (n=14). Single leg knee extension exercise was used to quantify peak leg blood flow (Doppler ultrasound), arterial-to-venous oxygen content difference (femoral venous catheter), leg VO2, and muscle oxygen diffusive conductance. In a subset of participants (n=36), phosphocreatine recovery time was measured by magnetic resonance spectroscopy to determine skeletal muscle oxidative capacity.
Results: Peak VO2 during cardiopulmonary exercise testing was not different between groups (central: 13.9±5.7 versus peripheral: 12.0±3.1 mL/min per kg; P=0.135); however, the peripheral group had a lower peak arterial-to-venous oxygen content difference (central: 13.5±2.0 versus peripheral: 11.1±1.6 mLO2/dL blood; P<0.001). During single leg knee extension, there was no difference in peak leg VO2 (P=0.306), but the peripherally limited group had greater blood flow/VO2 ratio (P=0.024), lower arterial-to-venous oxygen content difference (central: 12.3±2.5 versus peripheral: 10.3±2.2 mLO2/dL blood; P=0.013), and lower muscle oxygen diffusive conductance (P=0.021). A difference in magnetic resonance spectroscopy-derived phosphocreatine recovery time was not detected (P=0.199).
Conclusions: Peripherally limited patients with heart failure with preserved ejection fraction identified by cardiopulmonary exercise testing have impairments in oxygen transport and utilization at the level of the skeletal muscle quantified by invasive knee extension exercise testing, which includes an increased blood flow/V̇O2 ratio and poor muscle diffusive capacity.
Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT04068844.
Keywords: exercise test; heart failure; magnetic resonance imaging; muscle, skeletal; stroke volume.
Conflict of interest statement
None.
Figures

References
-
- Wilson JR, et al. , Relationship between exertional symptoms and functional capacity in patients with heart failure. J Am Coll Cardiol, 1999. 33(7): p. 1943–7. - PubMed
-
- Borlaug BA, Mechanisms of exercise intolerance in heart failure with preserved ejection fraction. Circ J, 2014. 78(1): p. 20–32. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
