

Circulating Tumor DNA Assay Detects Merkel Cell Carcinoma Recurrence, Disease Progression, and Minimal Residual Disease: Surveillance and Prognostic Implications
- PMID: 39052958
- PMCID: PMC11379364
- DOI: 10.1200/JCO.23.02054
Circulating Tumor DNA Assay Detects Merkel Cell Carcinoma Recurrence, Disease Progression, and Minimal Residual Disease: Surveillance and Prognostic Implications
Abstract
Purpose: Merkel cell carcinoma (MCC) is an aggressive skin cancer with a 40% recurrence rate, lacking effective prognostic biomarkers and surveillance methods. This prospective, multicenter, observational study aimed to evaluate circulating tumor DNA (ctDNA) as a biomarker for detecting MCC recurrence.
Methods: Plasma samples, clinical data, and imaging results were collected from 319 patients. A tumor-informed ctDNA assay was used for analysis. Patients were divided into discovery (167 patients) and validation (152 patients) cohorts. Diagnostic performance, including sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV), was assessed.
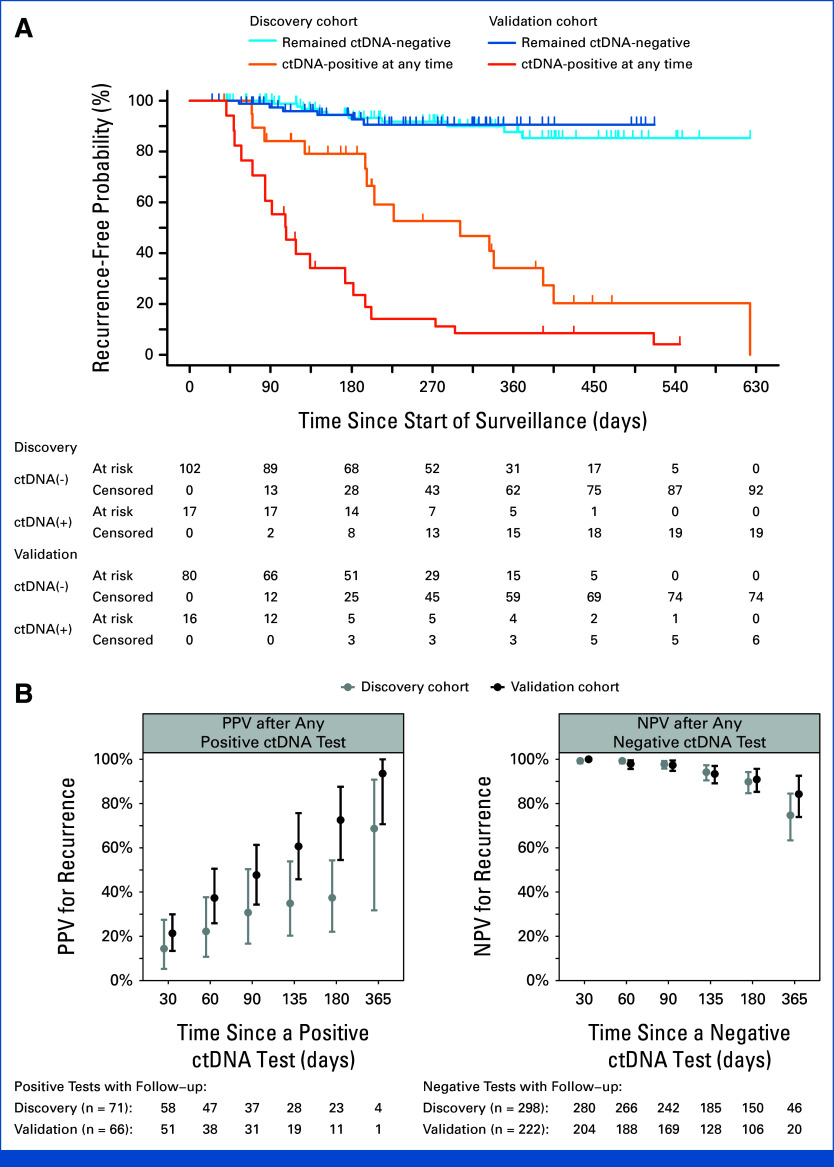
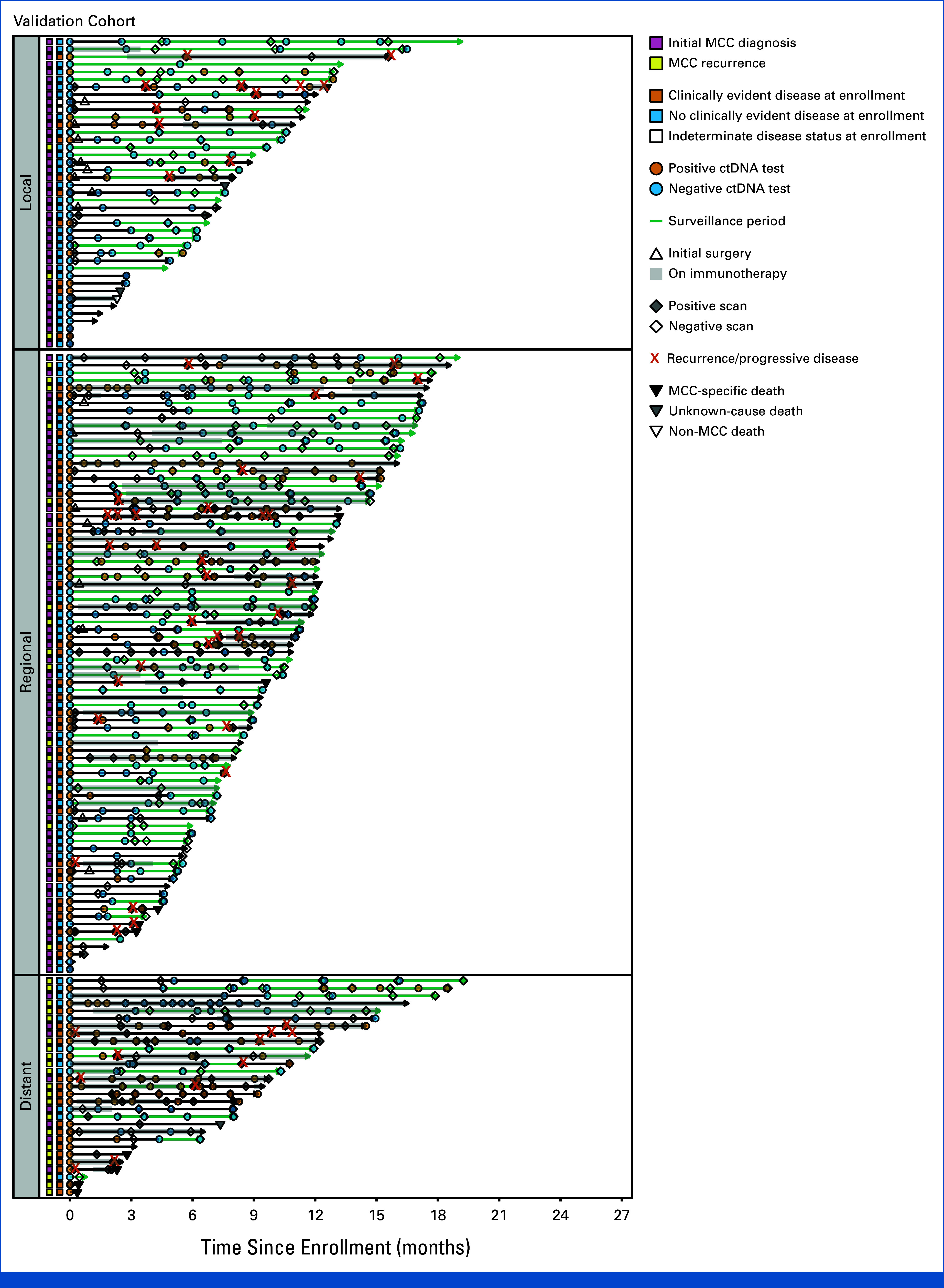
Results: ctDNA showed high sensitivity, 95% (discovery; 95% CI, 87 to 99) and 94% (validation; 95% CI, 85 to 98), for detecting disease at enrollment, with corresponding specificities of 90% (95% CI, 82 to 95) and 86% (95% CI, 77 to 93). A positive ctDNA during surveillance indicated increased recurrence risk, with hazard ratios (HRs) of 6.8 (discovery; 95% CI, 2.9 to 16) and 20 (validation; 95% CI, 8.3 to 50). The PPV for clinical recurrence at 1 year after a positive ctDNA test was 69% (discovery; 95% CI, 32 to 91) and 94% (validation; 95% CI, 71 to 100), respectively. The NPV at 135 days after a negative ctDNA test was 94% (discovery; 95% CI, 90 to 97) and 93% (validation; 95% CI, 89 to 97), respectively. Patients positive for ctDNA within 4 months after treatment had higher rates of recurrence, with 1-year rates of 74% versus 21% (adjusted HR, 7.4 [95% CI, 2.7 to 20]).
Conclusion: ctDNA testing exhibited high prognostic accuracy in detecting MCC recurrence, suggesting its potential to reduce frequent surveillance imaging. ctDNA also identifies high-risk patients who need more frequent imaging and may be best suited for adjuvant therapy trials.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
No other potential conflicts of interest were reported.
Figures










References
-
- Network NCC. Merkel cell carcinoma (version 1.2023). https://www.nccn.org/professionals/physician_gls/pdf/mcc.pdf
