

Metformin exposure and the incidence of lactic acidosis in critically ill patients with T2DM: A retrospective cohort study
- PMID: 39053014
- PMCID: PMC11282515
- DOI: 10.1177/00368504241262116
Metformin exposure and the incidence of lactic acidosis in critically ill patients with T2DM: A retrospective cohort study
Abstract
Objective: The objective of this study was to investigate the correlation between metformin exposure and the incidence of lactic acidosis in critically ill patients.
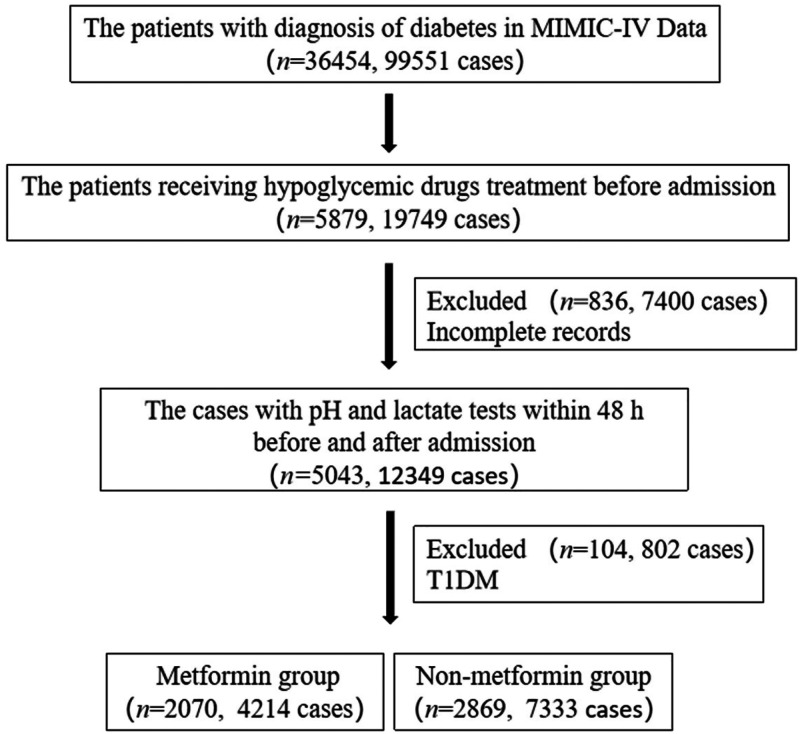
Methods: The patients with type 2 diabetes mellitus (T2DM) were included from Medical Information Mart for Intensive Care IV database (MIMIC-IV). The primary outcome was the incidence of lactic acidosis. The secondary outcomes were lactate level and in-hospital mortality. Propensity score matching (PSM) method was adopted to reduce bias of the confounders. The multivariate logistic regression was used to explore the correlation between metformin exposure and the incidence of lactic acidosis. Subgroup analysis and sensitivity analysis were used to test the stability of the conclusion.
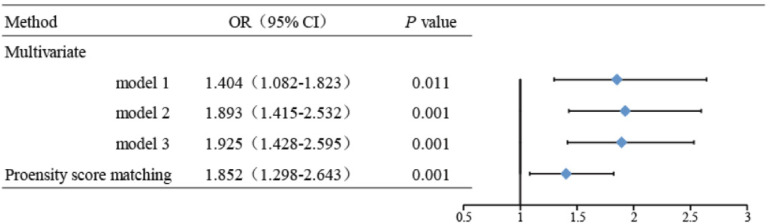
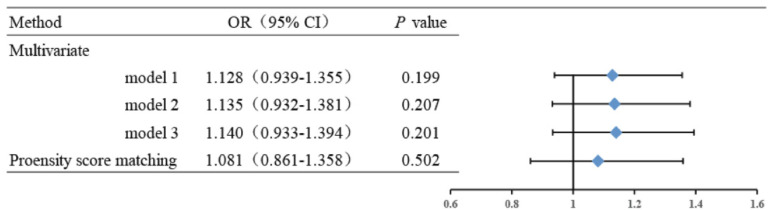
Results: We included 4939 patients. There were 2070 patients in the metformin group, and 2869 patients in the nonmetformin group. The frequency of lactic acidosis was 5.7% (118/2070) in the metformin group and it was 4.3% (122/2869) in the nonmetformin group. There was a statistically significant difference between the two groups (P < 0.05). The lactate level in the metformin group was higher than in the nonmetformin group (2.78 ± 2.23 vs. 2.45 ± 2.24, P < 0.001). After PSM, the frequency of lactic acidosis (6.3% vs. 3.7%, P < 0.001) and lactate level (2.85 ± 2.38 vs. 2.40 ± 2.14, P < 0.001) were significantly higher in the metformin group compared with the nonmetformin group. In multivariate logistic models, the frequency of lactic acidosis was obviously increased in metformin group, and the adjusted odds ratio (OR) of metformin exposure was 1.852 (95% confidence interval (CI) = 1.298-2.643, P < 0.001). The results were consistent with subgroup analysis except for respiratory failure subgroup. Metformin exposure increased lactate level but did not affect the frequency of lactic acidosis in patients of respiratory failure with hypercapnia. However, the in-hospital mortality between metformin and nonmetformin group had no obvious difference (P = 0.215). In sensitivity analysis, metformin exposure showed similar effect as the original cohort.
Conclusions: In critically ill patients with T2DM, metformin exposure elevated the incidence of lactic acidosis except for patients of respiratory failure with hypercapnia, but did not affect the in-hospital mortality.
Keywords: Metformin; critically ill patients; lactic acidosis; type 2 diabetes mellitus.
Conflict of interest statement
Declaration of conflicting interestsThe authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Li JZ, Li YR. Cardiovascular protection by metformin: latest advances in basic and clinical research. Cardiology 2023; 148: 374–384. - PubMed
-
- Maruthur NM, Tseng E, Hutfless S, et al. Diabetes medications as monotherapy or metformin-based combination therapy for type 2 diabetes: a systematic review and meta-analysis. Ann Intern Med 2016; 164: 740–751. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
