

Pembrolizumab with platinum-based chemotherapy with or without epacadostat as first-line treatment for metastatic non-small cell lung cancer: a randomized, partially double-blind, placebo-controlled phase II study
- PMID: 39054462
- PMCID: PMC11270757
- DOI: 10.1186/s12885-022-10427-4
Pembrolizumab with platinum-based chemotherapy with or without epacadostat as first-line treatment for metastatic non-small cell lung cancer: a randomized, partially double-blind, placebo-controlled phase II study
Abstract
Background: The combination of the checkpoint inhibitor (CPI) pembrolizumab and platinum-based chemotherapy is effective frontline therapy for advanced non-small cell lung cancer (NSCLC) lacking targetable mutations. Indoleamine 2,3- dioxygenase 1 (IDO1), an enzyme involved in kynurenine production, inhibits immune responses. Inhibition of IDO1 may restore antitumor immunity and augment CPI activity. This trial evaluated addition of epacadostat, a potent and highly selective IDO1 inhibitor, to pembrolizumab and chemotherapy for metastatic NSCLC.
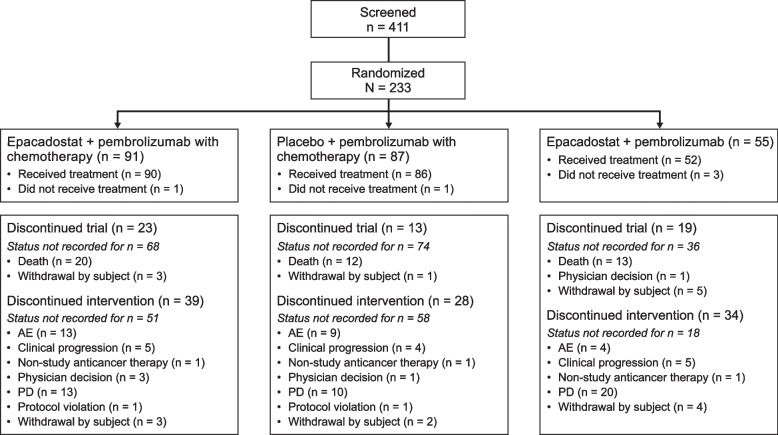
Methods: ECHO-306/KEYNOTE-715 was a partial double-blind, randomized phase II study of adults with treatment-naïve stage IV NSCLC not indicated for EGFR-, ALK-, or ROS1-directed therapy. Patients were randomized to one of three treatment arms: epacadostat-pembrolizumab-chemotherapy (E + P + C; blinded), epacadostat-pembrolizumab (E + P; open-label) or placebo-pembrolizumab-chemotherapy (PBO + P + C; blinded). Stratification was by PD-L1 tumor proportion score (< 50% vs. ≥ 50%) and tumor histology (non-squamous vs. squamous). A protocol amendment closed enrollment in the open-label E + P group, excluding it from efficacy analyses. Intravenous pembrolizumab (200 mg) was administered every 21 days and epacadostat 100 mg or matching placebo (oral) twice daily (BID) for ≤ 35 3-week cycles. The primary objective was objective response rate (ORR) for E + P + C vs. PBO + P + C.
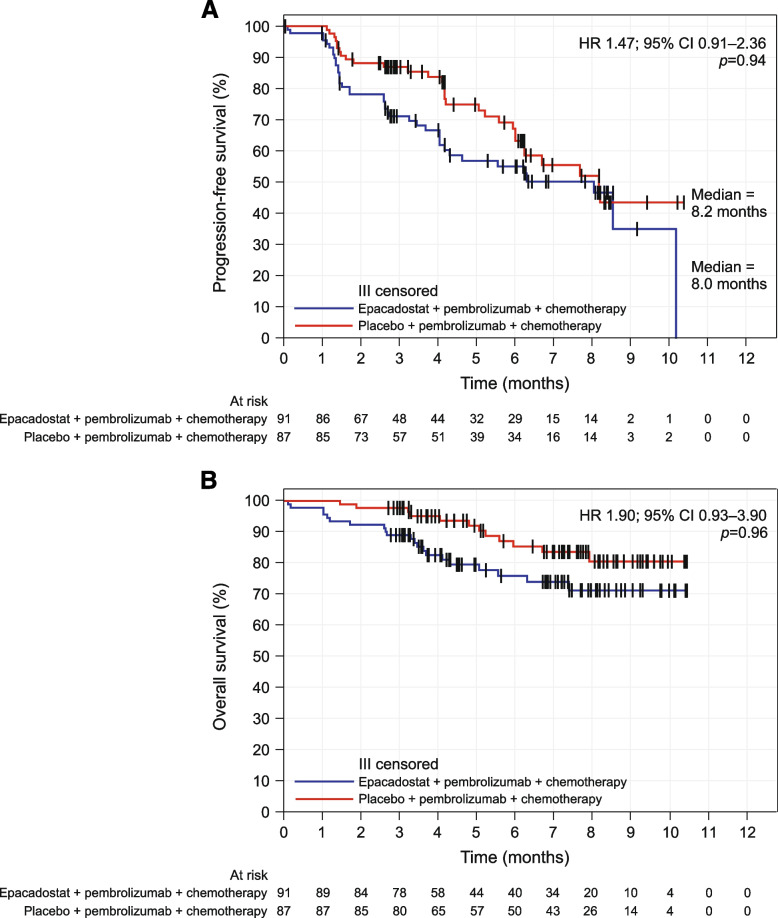
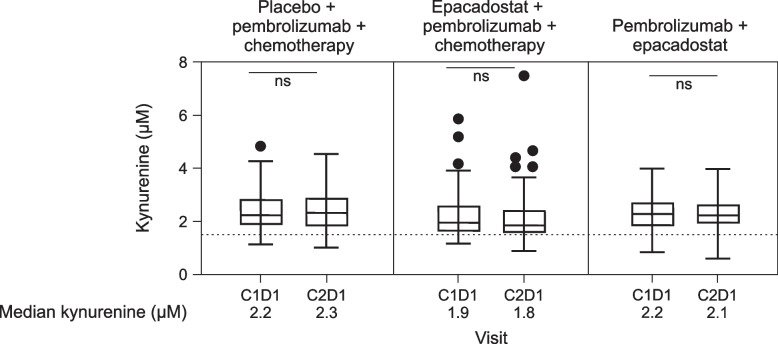
Results: 178 patients were randomized to E + P + C (n = 91) or PBO + P + C (n = 87); 55 were enrolled in the E + P group. The E + P + C group had a lower confirmed ORR (26.4%; 95% CI 17.7-36.7) than the PBO + P + C group (44.8%; 95% CI 34.1-55.9), with a difference of - 18.5% (95% CI - 32.0 - (- 4.3); one-sided P = 0.9948). The E + P + C group had a numerically higher percentage of confirmed responders with extended response ≥ 6 months (29.2% vs. 15.4%). Circulating kynurenine levels at C1D1 were similar to those at C2D1 in all treatment groups and were not reduced to normal levels with epacadostat 100 mg BID plus P + C. The safety profile of E + P + C was consistent with that for PBO + P + C.
Conclusions: Addition of epacadostat 100 mg BID to pembrolizumab and platinum-based chemotherapy was generally well tolerated but did not improve ORR in patients with treatment-naïve metastatic NSCLC. Evaluating epacadostat doses that normalize circulating kynurenine in combination with CPIs may help determine the clinical potential of this combination.
Trial registration: NCT03322566. Registered October 26, 2017.
Keywords: Combination immunotherapy; Epacadostat; Non-small cell lung cancer; Pembrolizumab.
© 2023. The Author(s).
Conflict of interest statement
MB reports institutional research funding from Amgen, AstraZeneca, BeiGene, Ltd., Boehringer Ingelheim, Bristol-Myers Squibb, Genentech/Roche, Merck Sharpe & Dohme, and Pfizer; and advisory board participation for AstraZeneca, Bristol-Myers Squibb, Merck Sharpe & Dohme, and Roche. RH reports advisory board participation for AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Merck Sharp & Dohme, Novartis, Pfizer, Roche and Seagen; and speaker honoraria from Merck Sharp & Dohme, Novartis and Roche. DU reports honoraria from AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Merck Sharp & Dohme (Israel), Roche, and Takeda; consultancy for Merck Sharp & Dohme (Israel), Roche, and Takeda; and other (travel) for AstraZeneca and Takeda. PC and W–CS have nothing to disclose. CD reports advisory committee participation for Bristol-Myers Squibb and Merck. SG reports personal fees from Blueprint, Roche/Genentech, AstraZeneca, Janssen, Bristol Myers-Squibb, Pfizer, Eli Lilly, Novartis, and Daichii; grants and personal fees from Merck; and a role on the IDMC of a phase III trial sponsored by AstraZeneca. MG reports honoraria from AstraZeneca/MedImmune, Bristol-Myers Squibb, GlaxoSmithKline, MSD Oncology, Roche, and Takeda; consulting or advisory roles with AstraZeneca, Bayer, Blueprint Medicines, Bristol-Myers Squibb, Celgene, Daichii Sankyo, GlaxoSmithKline, Incyte, Inivata, Janssen, Lilly, MSD, Novartis, Pfizer, Regeneron, Roche, Sanofi, Seattle Genetics, Takeda, and Tiziana Life Sciences; Speakers’ Bureau participation with AstraZeneca, Bristol-Myers Squibb, Celgene, Incyte, Lilly, MSD Oncology, Otsuka, Roche, and Takeda; and research funding from Amgen (Inst), AstraZeneca (Inst), AstraZeneca/MedImmune (Inst), Blueprint Medicines (Inst), Bristol-Myers Squibb (Inst), Exelixis (Inst), GlaxoSmithKline (Inst), Incyte (Inst), Ipsen (Inst), Janssen (Inst), Lilly (Inst), MedImmune (Inst), Merck (Inst), MSD (Inst), Novartis (Inst), Pfizer (Inst), Roche/Genentech (Inst), Sanofi (Inst), Spectrum Pharmaceuticals (Inst), and Takeda (Inst); and travel/accommodation/expenses from AstraZeneca, Pfizer, and Roche. LL, MCM, and JD are salaried employees of and own stock in Incyte Corporation. AS and YL are salaried employees of Merck & Co., Inc., Rahway, NJ, USA and own stock in the Company. DRA reports personal fees/honoraria for consultancy and lectures from Roche, AstraZeneca, Bristol-Myers Squibb, Merck Sharp & Dohme, Eli Lilly, Pfizer, and Novartis; travel expenses from Roche, Bristol-Myers Squibb, Merck Sharp & Dohme, and Novartis; and grant support for institutional studies from Bristol-Myers Squibb.
Figures
References
-
- American Cancer Society. Cancer Facts & Figures 2023. Atlanta: American Cancer Society; 2023.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
