

Blood pressure response index and clinical outcomes in patients with septic shock: a multicenter cohort study
- PMID: 39059317
- PMCID: PMC11338059
- DOI: 10.1016/j.ebiom.2024.105257
Blood pressure response index and clinical outcomes in patients with septic shock: a multicenter cohort study
Abstract
Background: Sepsis is a leading cause of mortality in intensive care units and vasoactive drugs are widely used in septic patients. The cardiovascular response of septic shock patients during resuscitation therapies and the relationship of the cardiovascular response and clinical outcome has not been clearly described.
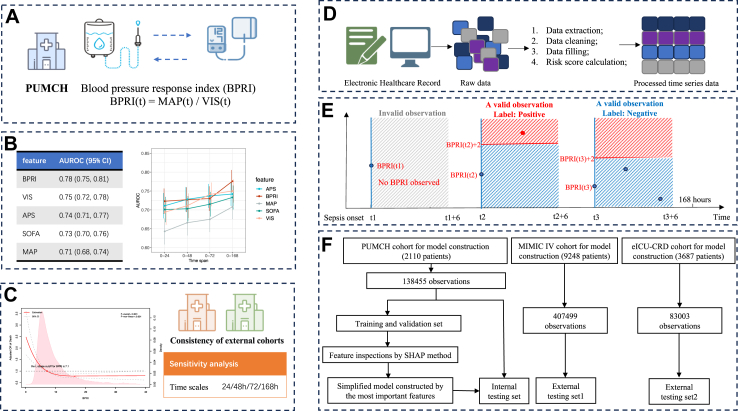
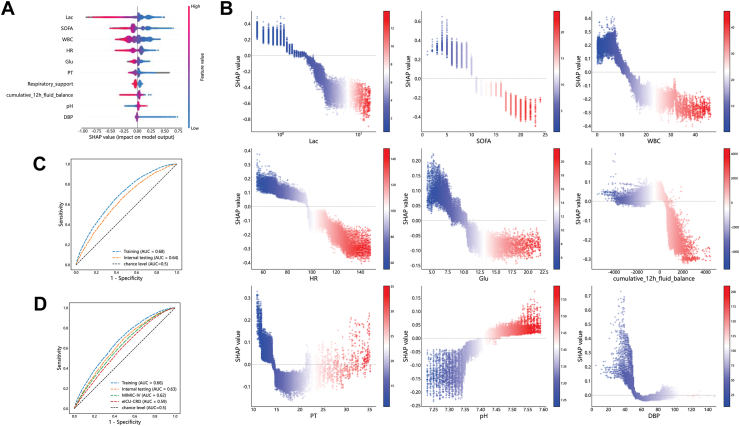
Methods: We included adult patients admitted to the ICU with sepsis from Peking Union Medical College Hospital (internal), Medical Information Mart for Intensive Care IV (MIMIC-IV) and eICU Collaborative Research Database (eICU-CRD). The Blood Pressure Response Index (BPRI) was defined as the ratio between the mean arterial pressure and the vasoactive-inotropic score. BRRI was compared with existing risk scores on predicting in-hospital death. The relationship between BPRI and in-hospital mortality was calculated. A XGBoost's machine learning model identified the features that influence short-term changes in BPRI.
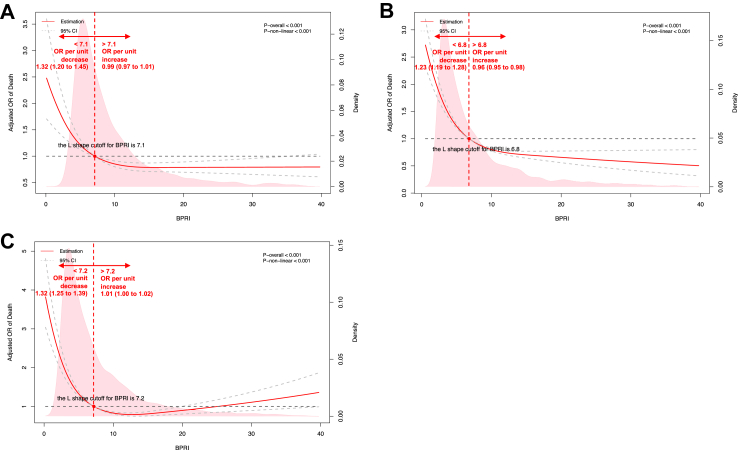
Findings: There were 2139, 9455, and 4202 patients in the internal, MIMIC-IV and eICU-CRD cohorts, respectively. BPRI had a better AUROC for predicting in-hospital mortality than SOFA (0.78 vs. 0.73, p = 0.01) and APS (0.78 vs. 0.74, p = 0.03) in the internal cohort. The estimated odds ratio for death per unit decrease in BPRI was 1.32 (95% CI 1.20-1.45) when BPRI was below 7.1 vs. 0.99 (95% CI 0.97-1.01) when BPRI was above 7.1 in the internal cohort; similar relationships were found in MIMIC-IV and eICU-CRD. Respiratory support and latest cumulative 12-h fluid balance were intervention-related features influencing BPRI.
Interpretation: BPRI is an easy, rapid, precise indicator of the response of patients with septic shock to vasoactive drugs. It is a comparable and even better predictor of prognosis than SOFA and APS in sepsis and it is simpler and more convenient in use. The application of BPRI could help clinicians identify potentially at-risk patients and provide clues for treatment.
Funding: Fundings for the Beijing Municipal Natural Science Foundation; the National High Level Hospital Clinical Research Funding; the CAMS Innovation Fund for Medical Sciences (CIFMS) from Chinese Academy of Medical Sciences and the National Key R&D Program of China, Ministry of Science and Technology of the People's Republic of China.
Keywords: Dynamic risk model; Machine learning; Mortality; Septic shock; Vascular reactivity.
Copyright © 2024 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests All authors disclosed no potential conflict of interest.
Figures

References
-
- Demirhan S., Topcuoglu S., Karadag N., Ozalkaya E., Karatekin G. Vasoactive inotropic score as a predictor of mortality in neonatal septic shock. J Trop Pediatr. 2022;68(6) - PubMed
-
- Kelly R.P., Ting C.T., Yang T.M., et al. Effective arterial elastance as index of arterial vascular load in humans. Circulation. 1992;86(2):513–521. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
