

Alliance A022104/NRG-GI010: The Janus Rectal Cancer Trial: a randomized phase II/III trial testing the efficacy of triplet versus doublet chemotherapy regarding clinical complete response and disease-free survival in patients with locally advanced rectal cancer
- PMID: 39060961
- PMCID: PMC11282593
- DOI: 10.1186/s12885-024-12529-7
Alliance A022104/NRG-GI010: The Janus Rectal Cancer Trial: a randomized phase II/III trial testing the efficacy of triplet versus doublet chemotherapy regarding clinical complete response and disease-free survival in patients with locally advanced rectal cancer
Abstract
Background: Recent data have demonstrated that in locally advanced rectal cancer (LARC), a total neoadjuvant therapy (TNT) approach improves compliance with chemotherapy and increases rates of tumor response compared to neoadjuvant chemoradiation (CRT) alone. They further indicate that the optimal sequencing of TNT involves consolidation (rather than induction) chemotherapy to optimize complete response rates. Data, largely from retrospective studies, have also shown that patients with clinical complete response (cCR) after TNT may be managed safely with the watch and wait approach (WW) instead of preemptive total mesorectal resection (TME). However, the optimal consolidation chemotherapy regimen to achieve cCR has not been established, and a randomized clinical trial has not robustly evaluated cCR as a primary endpoint. Collaborating with a multidisciplinary oncology team and patient groups, we designed this NCI-sponsored study of chemotherapy intensification to address these issues and to drive up cCR rates, to provide opportunity for organ preservation, improve quality of life for patients and improve survival outcomes.
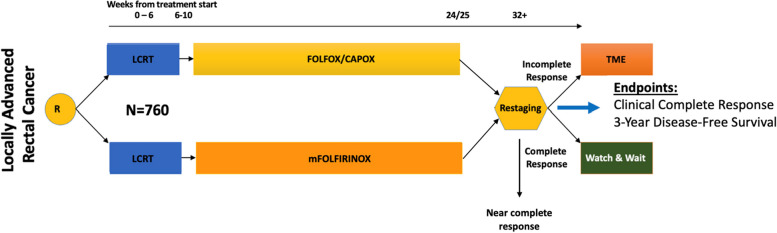
Methods: In this NCI-sponsored multi-group randomized, seamless phase II/III trial (1:1), up to 760 patients with LARC, T4N0, any T with node positive disease (any T, N +) or T3N0 requiring abdominoperineal resection or coloanal anastomosis and distal margin within 12 cm of anal verge will be enrolled. Stratification factors include tumor stage (T4 vs T1-3), nodal stage (N + vs N0) and distance from anal verge (0-4; 4-8; 8-12 cm). Patients will be randomized to receive neoadjuvant long-course chemoradiation (LCRT) followed by consolidation doublet (mFOLFOX6 or CAPOX) or triplet chemotherapy (mFOLFIRINOX) for 3-4 months. LCRT in both arms involves 4500 cGy in 25 fractions over 5 weeks + 900 cGy boost in 5 fractions with a fluoropyrimidine (capecitabine preferred). Patients will undergo assessment 8-12 (± 4) weeks post-TNT completion. The primary endpoint for the phase II portion will compare cCR between treatment arms. A total number of 312 evaluable patients (156 per arm) will provide statistical power of 90.5% to detect a 17% increase in cCR rate, at a one-sided alpha = 0.048. The primary endpoint for the phase III portion will compare disease-free survival (DFS) between treatment arms. A total of 285 DFS events will provide 85% power to detect an effect size of hazard ratio 0.70 at a one-sided alpha of 0.025, requiring enrollment of 760 patients (380 per arm). Secondary objectives include time-to event outcomes (overall survival, organ preservation time and time to distant metastasis) and adverse event rates. Biospecimens including archival tumor tissue, plasma and buffy coat, and serial rectal MRIs will be collected for exploratory correlative research. This study, activated in late 2022, is open across the NCTN and had accrued 330 patients as of May 2024. Study support: U10CA180821, U10CA180882, U24 CA196171; https://acknowledgments.alliancefound.org .
Discussion: Building on data from modern day rectal cancer trials and patient input from national advocacy groups, we have designed The Janus Rectal Cancer Trial studying chemotherapy intensification via a consolidation chemotherapy approach with the intent to enhance cCR and DFS rates, increase organ preservation rates, and improve quality of life for patients with rectal cancer.
Trial registration: Clinicaltrials.gov ID: NCT05610163; Support includes U10CA180868 (NRG) and U10CA180888 (SWOG).
Keywords: Clinical complete response; Locally advanced rectal cancer; Organ preservation; Total neoadjuvant therapy; Watch and wait/active surveillance.
© 2024. The Author(s).
Conflict of interest statement
JA declare that they have no competing interests.
QS reports consulting/advisory role from Yiviva Inc, Boehringer Ingelheim Pharmaceuticals, Inc, Regeneron Pharmaceuticals, Inc., Hoosier Cancer Research Network, Kronos Bio, and Mirati Therapeutics Inc; Honorarium/speaker role from Chugai Pharmaceutical Co., Ltd (to myself), research funds from Celgene/BMS, Roche/Genentech, Janssen, Novartis (to institution).
AD reports grants or contracts from HUTCHMED International Corporation, Eisai and Crinetics; consulting fees from HUTCHMED, Crinetics, and AAA; and Advisory Board participation for Oncobay.
JGA claims ownership/equity interests for Intuitive Surgical Inc.
JGA serves as a consulting/advisory role for Medtronic, Intuitive Surgical, and Johnson & Johnson.
HS research funding: AstraZeneca, Roche, Amgen, Bristol-Myers Squibb, Pfizer, BioMed Valley Discoveries, Rgenix, Exelixis.
TJG reports consulting/advisory role from Pfizer/Array, Tempus Labs, and Billion To One and is supported by an NIH/NCI Cancer Center Support Grant (P30 CA247796) and an NIH/NCI NCI-sponsored Clinical Trial Research Specialist (R50 CA281930).
PP declare that they have no competing interests.
GN declare that they have no competing interests.
TA reports advisory role from AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Genentech.
OA reports a consulting or advisory role from Taiho Oncology, Pfizer, QED Therapeutics, Seagen, Bristol Myers Squibb, AADi, Seagen and research funding from Bristol-Myers Squibb, Ipsen, Taiho Pharmaceutical, Calithera Biosciences, Corcept Therapeutics, PCI Biotech, SynCoreBio, Hutchison MediPharma, GlaxoSmithKline, Transcenta.
WH declare that they have no competing interests.
DO declare that they have no competing interests.
FV declare that they have no competing interests.
AB declare that they have no competing interests.
MK declare that they have no competing interests.
JB declare that they have no competing interests.
HW declare that they have no competing interests.
MG declare that they have no competing interests.
RG declare that they have no competing interests.
PG declare that they have no competing interests.
EO reports research funding to institution: Genentech/Roche, BioNTech, AstraZeneca, Arcus, Elicio, Parker Institute, NIH/NCI, Digestive Care, Break Through Cancer and consulting/DSMB in Arcus, Alligator, Agenus, BioNTech, Ipsen, Merck, Moma Therapeutics, Novartis, Syros, Leap Therapeutics, Astellas, BMS, Fibrogen, Revolution Medicine, Merus Agios (spouse), Genentech-Roche (spouse), Eisai (spouse) Servier (Spouse).
JM declare that they have no competing interests.
NH declare that they have no competing interests.
PBR is an EMD Serono consultant and reports support for travel from Elekta and Philips Healthcare and prior research funding from EMD Serono.
JJS received travel support for fellow education from Intuitive Surgical (2015).
JJS served as a clinical advisor for Guardant Health (2019).
JJS served as a clinical advisor for Foundation Medicine (2022).
JJS served as a consultant and speaker for Johnson and Johnson (2022).
JJS serves as a clinical advisor and consultant for GSK (2023–24).
Figures
Update of
-
ALLIANCE A022104/NRG-GI010: The Janus Rectal Cancer Trial: a randomized phase II/III trial testing the efficacy of triplet versus doublet chemotherapy regarding clinical complete response and disease-free survival in patients with locally advanced rectal cancer.medRxiv [Preprint]. 2024 Apr 27:2024.04.25.24306396. doi: 10.1101/2024.04.25.24306396. medRxiv. 2024. Update in: BMC Cancer. 2024 Jul 26;24(1):901. doi: 10.1186/s12885-024-12529-7. PMID: 38712176 Free PMC article. Updated. Preprint.
References
-
- Bahadoer RR, Dijkstra EA, van Etten B, et al. Short-course radiotherapy followed by chemotherapy before total mesorectal excision (TME) versus preoperative chemoradiotherapy, TME, and optional adjuvant chemotherapy in locally advanced rectal cancer (RAPIDO): a randomised, open-label, phase 3 trial. Lancet Oncol. 2021;22(1):29–42. 10.1016/S1470-2045(20)30555-6. 10.1016/S1470-2045(20)30555-6 - DOI - PubMed
-
- Chau I, Brown G, Cunningham D, et al. Neoadjuvant capecitabine and oxaliplatin followed by synchronous chemoradiation and total mesorectal excision in magnetic resonance imaging–defined poor-risk rectal cancer. J Clin Oncol. Published online September 21, 2016. 10.1200/JCO.2005.04.4875 - PubMed
-
- Conroy T, Lamfichekh N, Etienne PL, et al. Total neoadjuvant therapy with mFOLFIRINOX versus preoperative chemoradiation in patients with locally advanced rectal cancer: Final results of PRODIGE 23 phase III trial, a UNICANCER GI trial. J Clin Oncol. 2020;38(15_suppl):4007–4007. 10.1200/JCO.2020.38.15_suppl.4007.10.1200/JCO.2020.38.15_suppl.4007 - DOI
-
- Fernandez-Martos C, Garcia-Albeniz X, Pericay C, et al. Chemoradiation, surgery and adjuvant chemotherapy versus induction chemotherapy followed by chemoradiation and surgery: long-term results of the Spanish GCR-3 phase II randomized trial†. Ann Oncol. 2015;26(8):1722–8. 10.1093/annonc/mdv223. 10.1093/annonc/mdv223 - DOI - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
