

Bizarre parosteal osteochondromatous proliferation in the distal ulna where the lesion is continuous with the medullary cavity: a case report
- PMID: 39061015
- PMCID: PMC11282834
- DOI: 10.1186/s12891-024-07715-4
Bizarre parosteal osteochondromatous proliferation in the distal ulna where the lesion is continuous with the medullary cavity: a case report
Abstract
Background: Bizarre parosteal osteochondromatous proliferation (BPOP) is a rare benign bone tumor, it is also called "Nora's lesion". The lesion is characterized by heterotopic ossification of the normal bone cortex or parosteal bone. The etiology of BPOP is unclear and may be related to trauma. In most BPOPs, the lesion is not connected to the medullary cavity. Here we report an atypical case, characterized by reversed features compared to the typical BPOP, which demonstrated continuity of the lesion with the cavity.
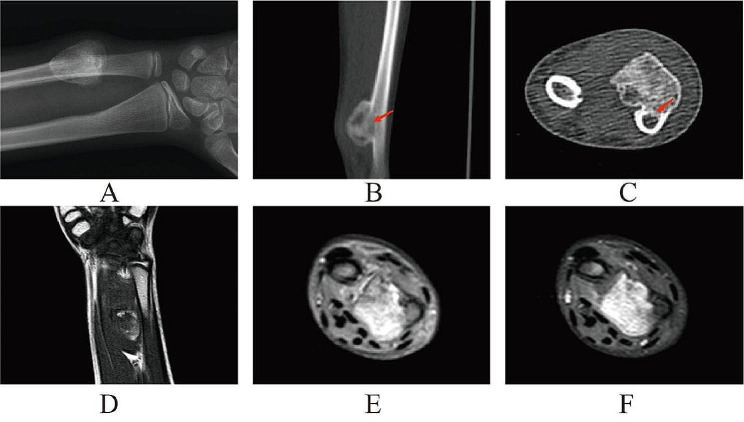
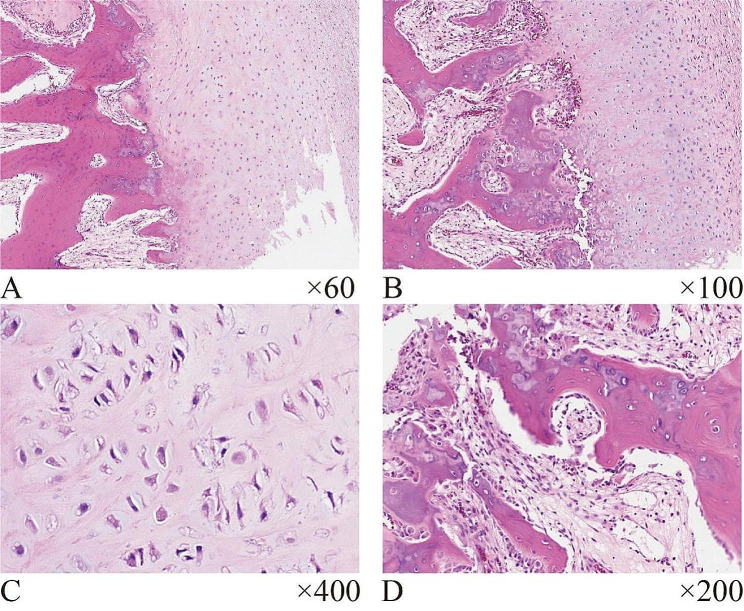
Case presentation: An 11-year-old female child had a slow-growing mass on her right wrist for 8 months with forearm rotation dysfunction. Plain X-rays showed an irregular calcified mass on the right distal ulna, and computed tomography (CT) showed a pedunculated mass resembling a mushroom protruding into the soft tissue at the distal ulna. The medulla of this lesion is continuous with the medulla of the ulna. A surgical resection of the lesion, together with a portion of the ulnar bone cortex below the tumor was performed, and the final pathology confirmed BPOP. After the surgery, the child's forearm rotation function improved significantly, and there was no sign of a recurrence at 1-year follow-up.
Conclusion: It is scarce for BPOP lesions to communicate with the medullary cavity. However, under-recognition of these rare cases may result in misdiagnosis or inappropriate treatment thereby increasing the risk of recurrence. Therefore, special cases where BPOP lesions are continuous with the medulla are even more important to be studied to understand better and master these lesions. Although BPOP is a benign tumor with no evidence of malignant transformation, the recurrence rate of surgical resection is high. We considered the possibility of this particular disease prior to surgery and performed a surgical resection with adequate safety margins. Regular postoperative follow-up is of utmost importance, without a doubt.
Keywords: Bizarre parosteal osteochondromatous proliferation; Continuity with the medullary cavity; Differential diagnosis; Nora’s lesion; Osteochondroma.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Grants and funding
- 82371600/the National Natural Science Foundation of China
- 2021JJ40810/the Natural Science Foundation of Hunan Province
- 2021JJ20086/the Natural Science Foundation of Hunan Province of Outstanding Young Scholars
- B202304077119/the Scientific Research Projects of the Health Commission of Hunan Province
- 22023JGB066/the Research Project on Teaching Reform of Postgraduate Education in Central South University
LinkOut - more resources
Full Text Sources
Medical
