

Predicting Aneurysmal Degeneration in Uncomplicated Residual Type B Aortic Dissection
- PMID: 39061772
- PMCID: PMC11274148
- DOI: 10.3390/bioengineering11070690
Predicting Aneurysmal Degeneration in Uncomplicated Residual Type B Aortic Dissection
Abstract
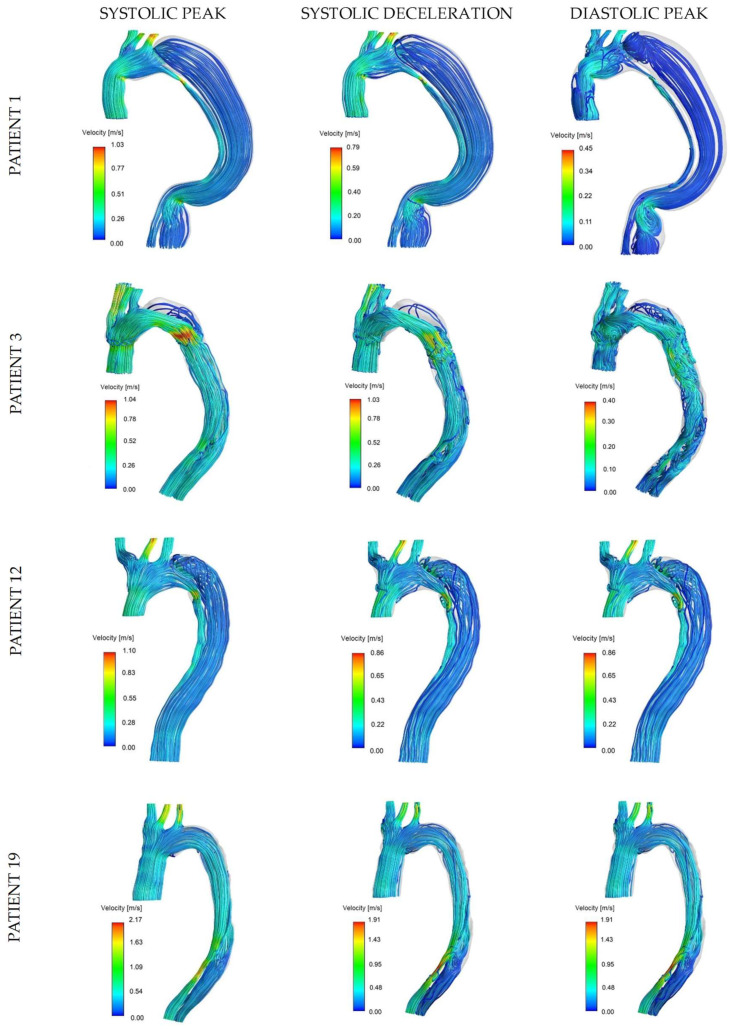
The formation of an aneurysm in the false lumen (FL) is a long-term complication in a significant percentage of type B aortic dissection (AD) patients. The ability to predict which patients are likely to progress to aneurysm formation is key to justifying the risks of interventional therapy. The investigation of patient-specific hemodynamics has the potential to enable a patient-tailored approach to improve prognosis by guiding disease management for type B dissection. CFD-derived hemodynamic descriptors and geometric features were used to retrospectively assess individual aortas for a population of residual type B AD patients and analyze correlations with known outcomes (i.e., rapid aortic growth, death). The results highlight great variability in flow patterns and hemodynamic descriptors. A rapid aortic expansion was found to be associated with a larger FL. Time-averaged wall shear stress at the tear region emerged as a possible indicator of the dynamics of flow exchange between lumens and its effect on the evolution of individual aortas. High FL flow rate and tortuosity were associated with adverse outcomes suggesting a role as indicators of risk. AD induces complex changes in vessel geometry and hemodynamics. The reported findings emphasize the need for a patient-tailored approach when evaluating uncomplicated type B AD patients and show the potential of CFD-derived hemodynamics to complement anatomical assessment and help disease management.
Keywords: CFD; aneurysmal degeneration; aortic dissection; hemodynamics.
Conflict of interest statement
A.F. and E.S.D.M are involved with the company ViTAA Medical Solutions.
Figures





References
-
- Erbel R., Alfonso F., Boileau C., Dirsch O., Eber B., Haverich A., Rakowski H., Struyven J., Radegran K., Sechtem U., et al. Diagnosis and management of aortic dissection: Task force on aortic dissection, european society of cardiology. Eur. Heart J. 2001;22:1642–1681. doi: 10.1053/euhj.2001.2782. - DOI - PubMed
-
- Isselbacher E.M., Preventza O., Hamilton Black J., III, Augoustides J.G., Beck A.W., Bolen M.A., Braverman A.C., Bray B.E., Brown-Zimmerman M.M., Chen E.P., et al. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease. J. Am. Coll. Cardiol. 2022;80:e223–e393. doi: 10.1016/j.jacc.2022.08.004. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
