

CARING: Cannula for Alleviation of Retinal Injury Caused by Needle Fluidic Gashing
- PMID: 39061799
- PMCID: PMC11274333
- DOI: 10.3390/bioengineering11070718
CARING: Cannula for Alleviation of Retinal Injury Caused by Needle Fluidic Gashing
Abstract
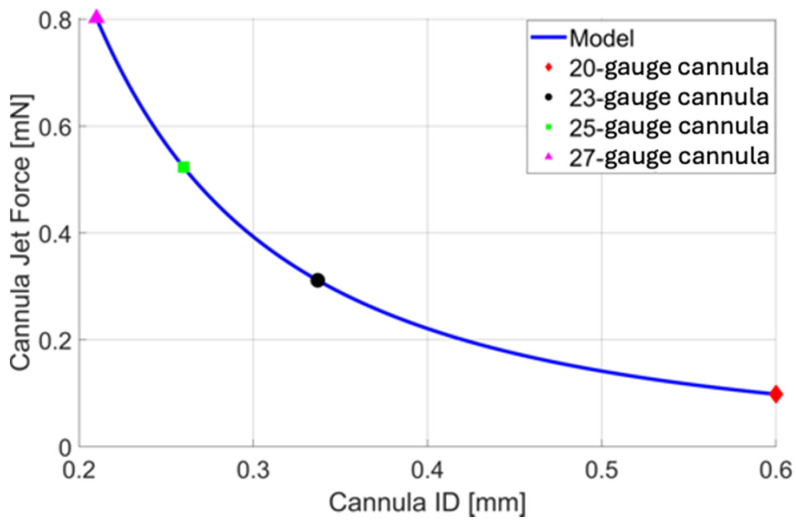
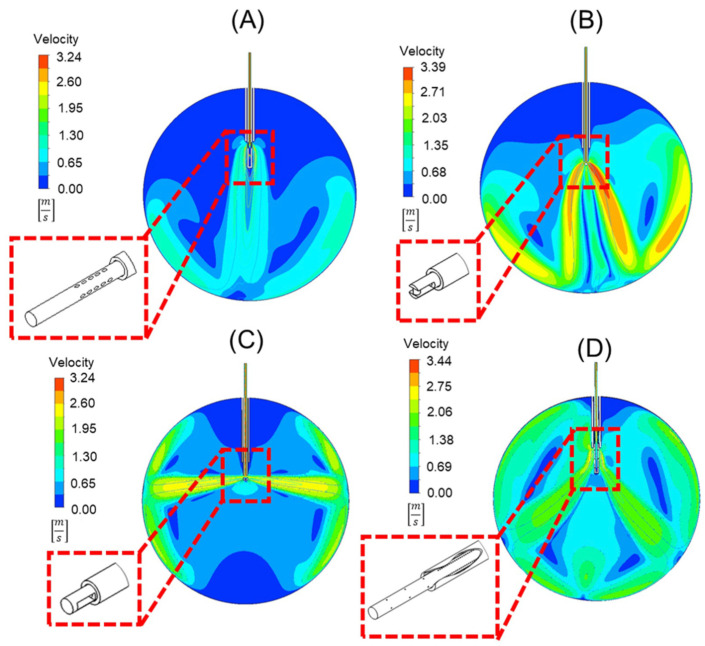
Infusion-related iatrogenic retinal breaks (IRBs) are a significant complication in vitrectomies, particularly when smaller-gauge cannulas are used during fluid infusion. Using two-dimensional finite element analysis (FEA), we analyzed forces exerted on the retina from different cannulas: traditional 25-gauge, 20-gauge, 23-gauge, and 27-gauge, then investigated four alternative new cannula designs: (A) oblique orifices, (B) external obstruction, (C) side ports, and (D) perpendicular orifices. The analysis revealed that the standard 25-gauge cannula had a force of 0.546 milli-Newtons (mN). Optimized cannulas demonstrated decreased forces: 0.072 mN (A), 0.266 mN (B), 0.417 mN (C), and 0.117 mN (D). While all the designs decrease fluid jet force, each has unique challenges: Design A may complicate manufacturing, B requires unique attachment techniques, C could misdirect fluid toward the lens and peripheral retina, and D requires a sealed trocar/cannula design to prevent unwanted fluid ejection. These four innovative cannula designs, identified with detailed engineering simulations, provide promising strategies to reduce the risk of IRBs during vitrectomy, bridging the gap between engineering insights and clinical application.
Keywords: cannula tip design; fluidic gashing; iatrogenic retinal breaks; infusion breaks.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
-
- Omari A., Mahmoud T.H. Vitrectomy. StatPearls Publishing; Treasure Island, FL, USA: 2020. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
