

Micromassage Compression Leggings Associated with Physical Exercise: Pilot Study and Example of Evaluation of the Clinical and Instrumental Effectiveness of Conservative Treatment in Lipedema
- PMID: 39063608
- PMCID: PMC11278218
- DOI: 10.3390/life14070854
Micromassage Compression Leggings Associated with Physical Exercise: Pilot Study and Example of Evaluation of the Clinical and Instrumental Effectiveness of Conservative Treatment in Lipedema
Abstract
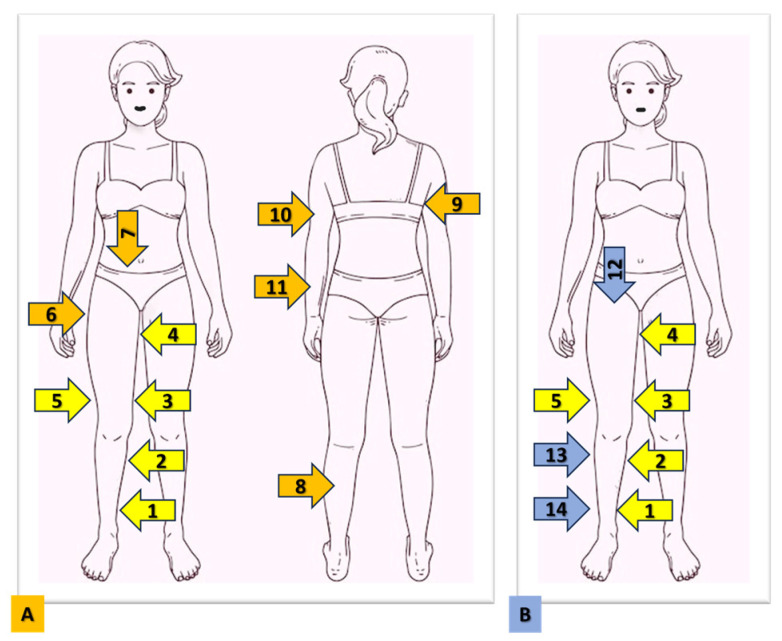
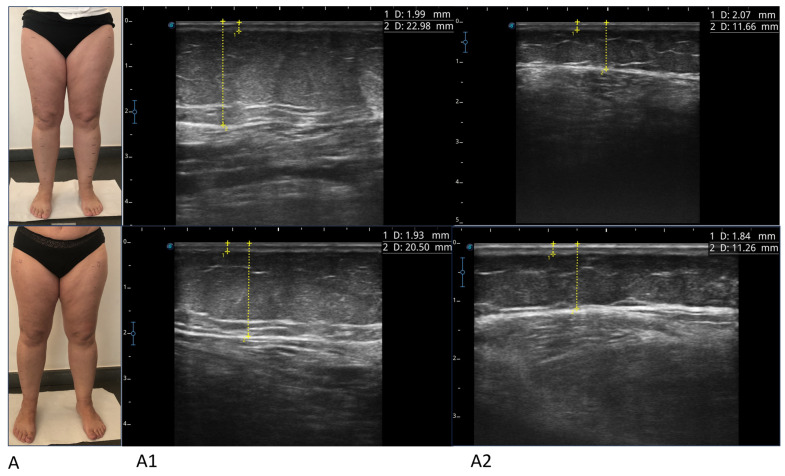
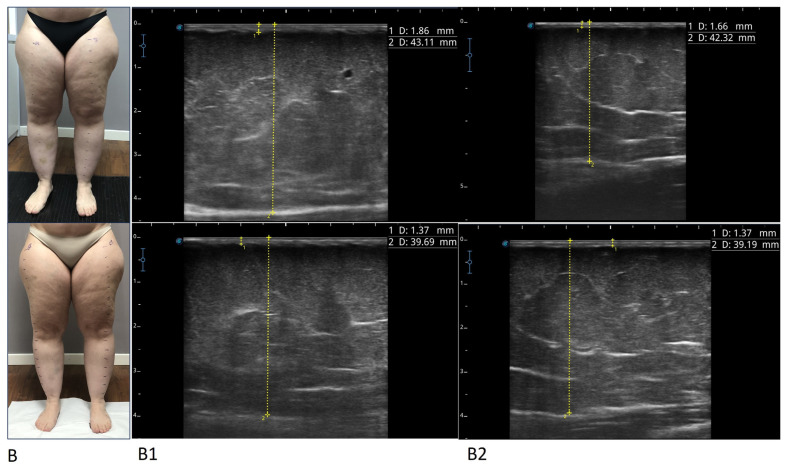
We evaluated the effect of compression leggings with micromassage in association with physical activity on women with lipedema, not previously treated and without recent changes in body weight. The treatment resulted in an improvement in all subjective parameters, in spontaneous and evoked pain, in the volume of the limbs, in the absence of significant changes in body weight, and regardless of the duration of use, age, years of illness, the clinical stage, and body mass index (BMI). Evoked pain did not improve in areas affected by untreated lipedema; foot circumferences did not increase. We found a significant reduction in the thickness of subcutaneous adipose tissue (SAT) and skin evaluated in multiple points of the lower limb. Micromassage compression leggings are proposed as an integral part of conservative treatment. A method is proposed for the clinical evaluation of evoked pain, called the Progressive Pain Check (PPC), which allows for the calculation of a numerical score called the Ricolfi-Patton Score (RPS) and for the ultrasound evaluation of tissues. The method is simple and repeatable and allows for completion of the clinical evaluation of the patient at diagnosis and for an evaluation of the effects of various treatments, even applied to just one side of the body.
Keywords: adipose tissue; compression; exercise; lipedema; micromassaging leggings; pain; treatment; ultrasound.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Alcolea J.M., Alonso A.B., Arroyo B.A., Domingo P., Garcia G.A., Graells G.M., Urraca I.C., Nipoti I.E., Castillo M.E., Alvarez M., Jr., et al. Consensus Document on Lipedema 2018. Includes Current Status of Lipedema 2019. LITOGAMA SL; Barcelona, Spain: 2018.
-
- Wounds UK Best. Practice Guidelines: The Management of Lipoedema. 2017. [(accessed on 28 August 2017)]. Available online: https://wounds-uk.com/bestpractice-statements/management-lipoedema/
LinkOut - more resources
Full Text Sources
Research Materials
