

High-Dose versus Low-Dose Oxytocin for Labor Augmentation: A Meta-Analysis of Randomized Controlled Trials
- PMID: 39063978
- PMCID: PMC11278403
- DOI: 10.3390/jpm14070724
High-Dose versus Low-Dose Oxytocin for Labor Augmentation: A Meta-Analysis of Randomized Controlled Trials
Abstract
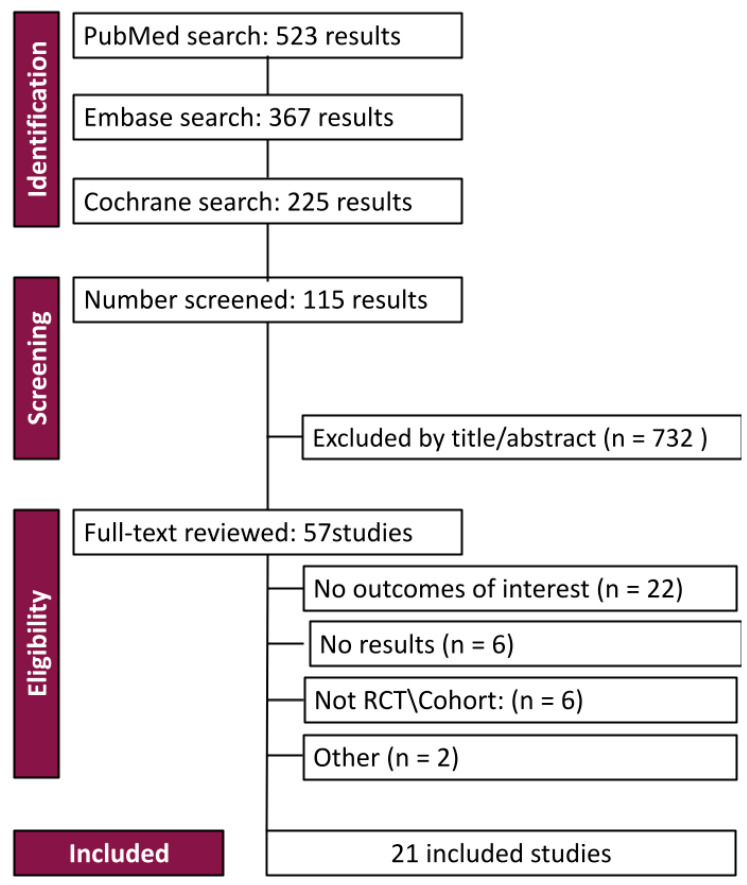
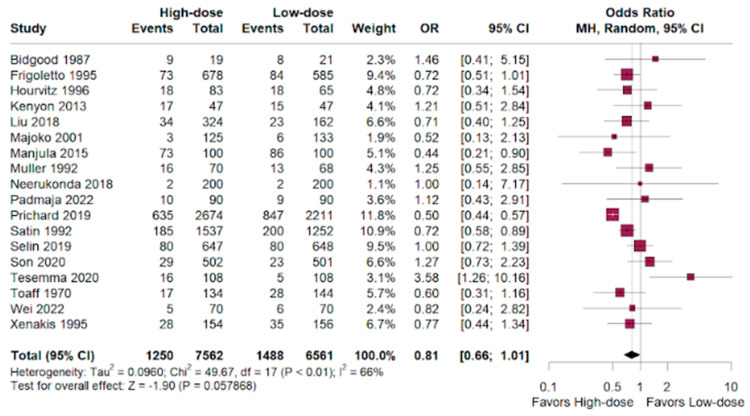
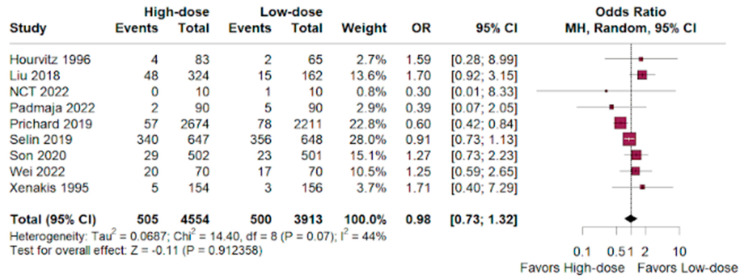
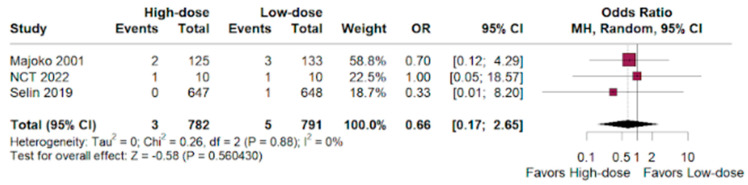
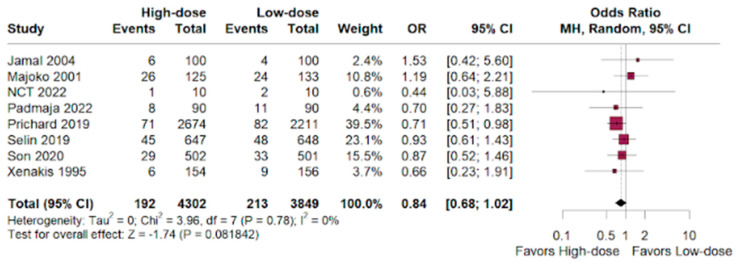
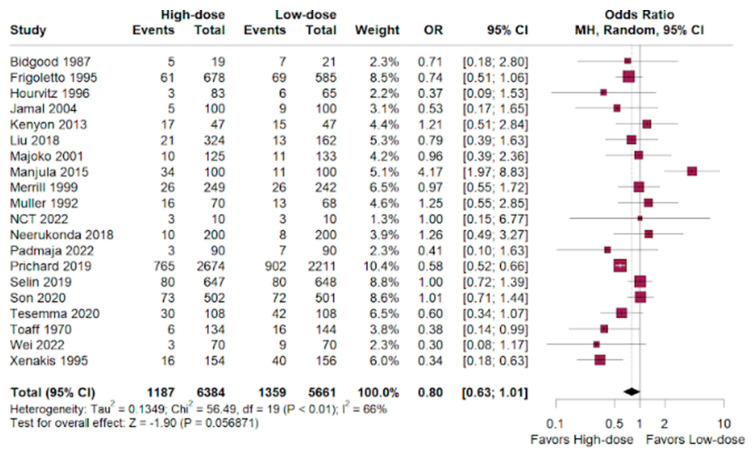
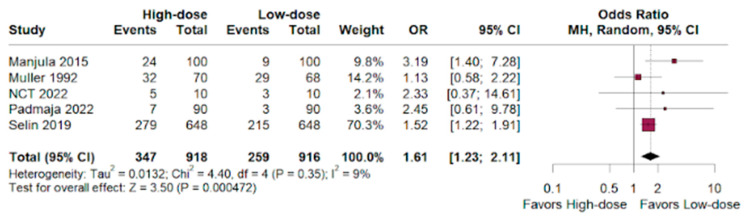
Background/Objectives: Although oxytocin administration is recommended for delayed labor progress, there is no consensus over the preferred optimal dose of oxytocin. We aimed to perform a meta-analysis of pregnancy outcomes comparing high-dose versus low-dose oxytocin regimens for augmentation of delayed labor. Methods: PubMed, Embase, and Cochrane databases were systematically searched for studies comparing high-dose with low-dose oxytocin for labor augmentation from inception up to May 2023. The outcomes assessed were cesarean rate, instrumental delivery rate, postpartum hemorrhage, neonatal death, and uterine tachysystole. Subgroup analysis was performed with randomized controlled trials (RCTs) and propensity-matched studies. Statistical analysis was performed using Rstudio. Heterogeneity was assessed with I2 statistics, and a random-risk effect was used if I2 > 50%. Results: Twenty-one studies met inclusion criteria, and eighteen were RCTs. A total of 14.834 patients were included, of whom 7.921 (53.3%) received high-dose and 6.913 (46.6%) received low-dose oxytocin during labor augmentation. No statistical differences were found in cesarean delivery, neonatal mortality, postpartum hemorrhage and vaginal instrumentation rate. However, uterine tachysystole incidence was significantly higher with high-dose oxytocin (95% Cl, 1.30-1.94, p = 0.3; 0.6; I2 = 9%). Conclusions: Labor augmentation with a low-dose oxytocin regimen is effective as with a high-dose regimen, but with significantly less uterine tachysystole events, which can lead to intrauterine and neonatal complications. Our findings suggest that a low-dose regimen may be safe and effective for labor augmentation in medical practice.
Keywords: high-dose; labor augmentation; low-dose; oxytocin.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Iovino M., Messana T., Tortora A., Giusti C., Lisco G., Giagulli V.A., Guastamacchia E., De Pergola G., Triggiani V. Oxytocin Signaling Pathway: From Cell Biology to Clinical Implications. Endocr. Metab. Immune Disord. Drug Targets. 2021;21:91–110. doi: 10.2174/1871530320666200520093730. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
