

Development of a Predictive Nomogram for Sepsis in Patients with Urolithiasis-Related Obstructive Pyelonephritis
- PMID: 39064542
- PMCID: PMC11279065
- DOI: 10.3390/medicina60071113
Development of a Predictive Nomogram for Sepsis in Patients with Urolithiasis-Related Obstructive Pyelonephritis
Abstract
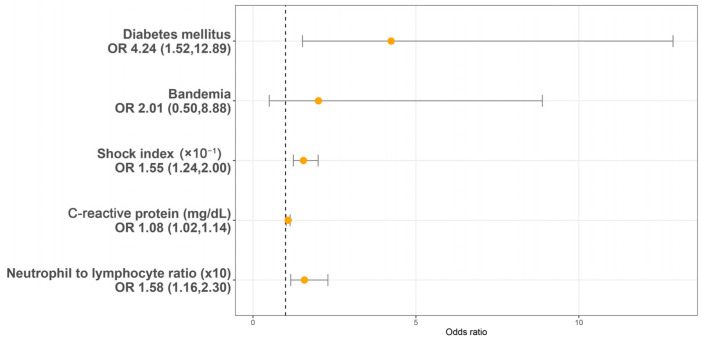
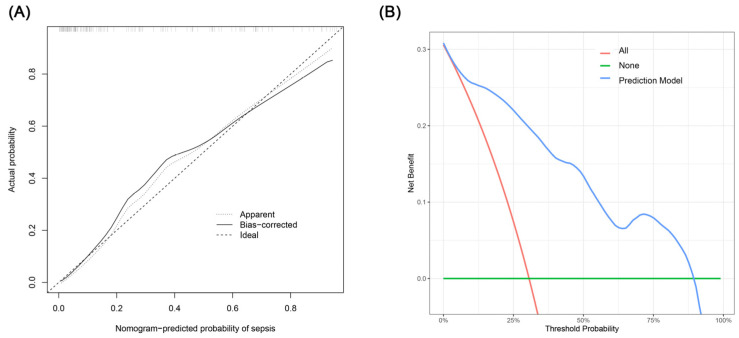
Background and Objectives: In patients with urolithiasis-related obstructive pyelonephritis (UROP), sepsis represents a critical and concerning complication that can substantially increase the mortality rate. This study aimed to identify the risk factors for sepsis in UROP patients and to develop a predictive nomogram model. Materials and Methods: We analyzed data from 148 patients who met the UROP criteria and were admitted to Chang Gung Memorial Hospital between 1 January 2016 and 31 December 2021. The primary outcome evaluated was the incidence of sepsis, as defined by the most recent Sepsis-3 guidelines. To identify potential risk factors for sepsis, we employed the Least Absolute Shrinkage and Selection Operator (LASSO) regression technique. Subsequently, we utilized multivariable logistic regression to construct the predictive model. Results: There was a total of 102 non-sepsis cases and 46 sepsis cases. Risk factors for sepsis in multivariable analysis were a history of diabetes mellitus (DM) (OR = 4.24, p = 0.007), shock index (SI) (×10-1) (OR = 1.55, p < 0.001), C-reactive protein (CRP) (mg/dL) (OR = 1.08, p = 0.005), and neutrophil to lymphocyte ratio (NLR) (×10) (OR = 1.58, p = 0.007). The nomogram exhibited an area under the receiver operating characteristic curve of 0.890 (95% CI 0.830-0.949). Conclusions: Our study demonstrated that patients with UROP who have DM, higher SI, higher NLR, and elevated CRP levels are significantly more likely to develop sepsis. These insights may aid in risk stratification, and it is imperative that clinicians promptly initiate treatment for those identified as high risk.
Keywords: nomogram; sepsis; uolithiasis-related obstructive pyelonephritis.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures



References
-
- Yamamichi F., Shigemura K., Kitagawa K., Fujisawa M. Comparison between non-septic and septic cases in stone-related obstructive acute pyelonephritis and risk factors for septic shock: A multi-center retrospective study. J. Infect. Chemother. 2018;24:902–906. doi: 10.1016/j.jiac.2018.08.002. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
