

The Safety Profile of Vitamin D Supplements Using Real-World Data from 445,493 Participants of the UK Biobank: Slightly Higher Hypercalcemia Prevalence but Neither Increased Risks of Kidney Stones nor Atherosclerosis
- PMID: 39064694
- PMCID: PMC11279740
- DOI: 10.3390/nu16142251
The Safety Profile of Vitamin D Supplements Using Real-World Data from 445,493 Participants of the UK Biobank: Slightly Higher Hypercalcemia Prevalence but Neither Increased Risks of Kidney Stones nor Atherosclerosis
Abstract
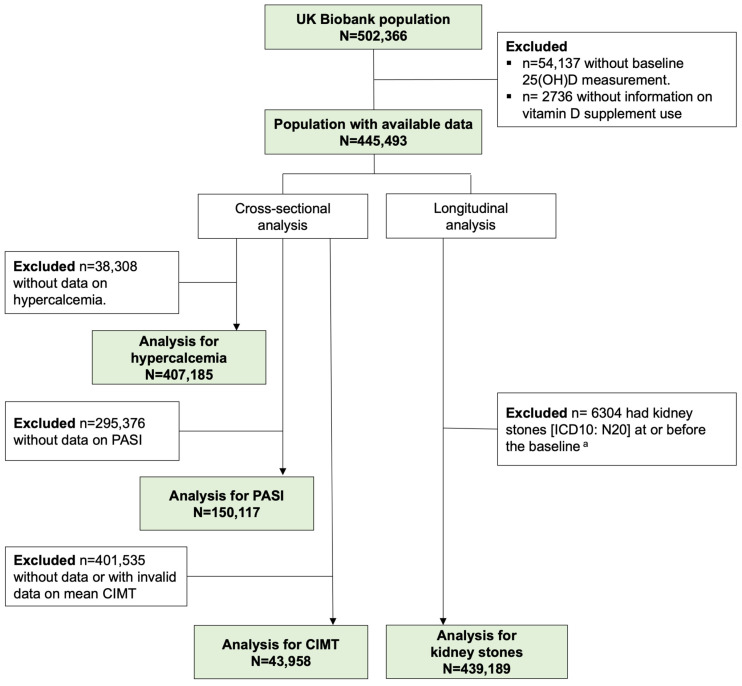
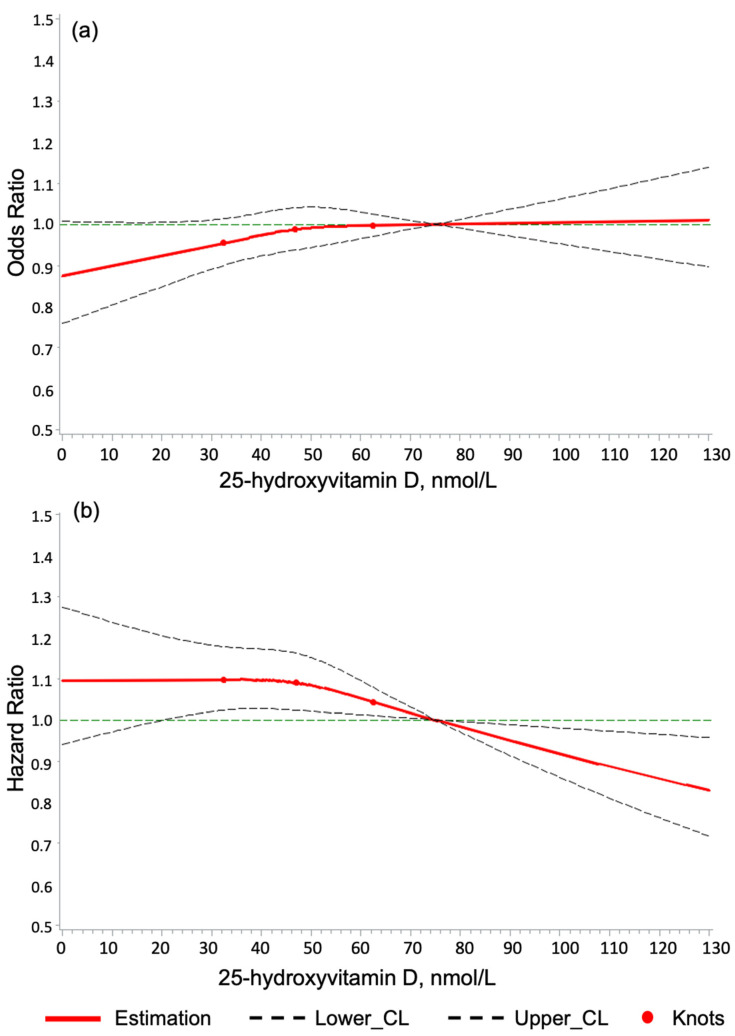
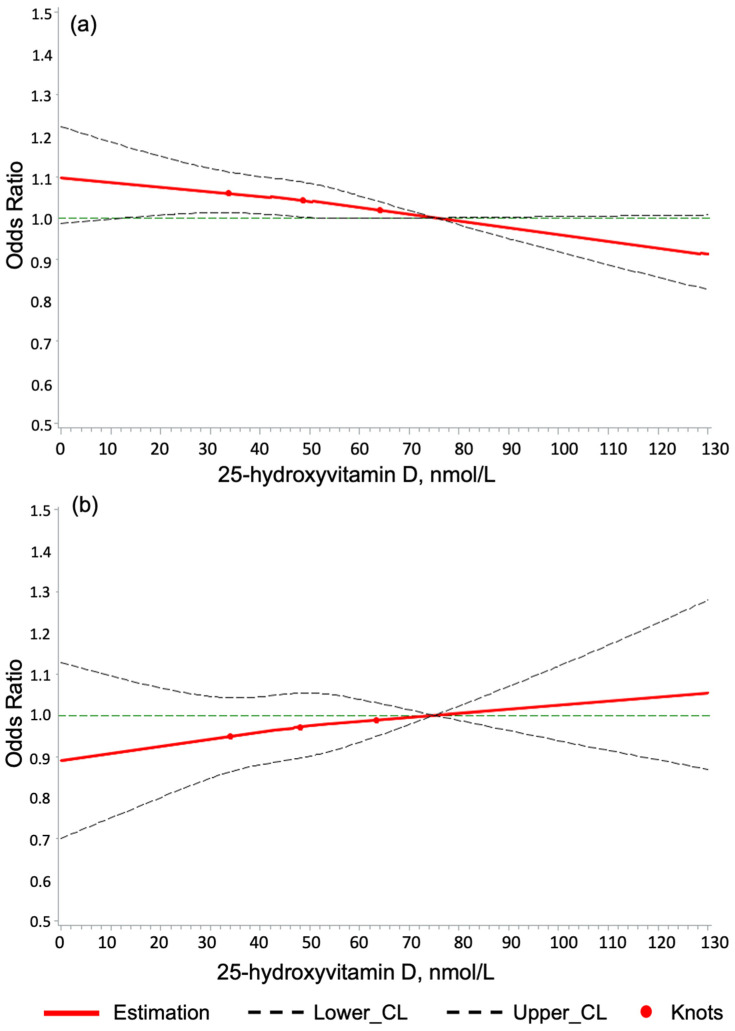
Background: Potential calcium-related adverse events of vitamin D supplement use have not been addressed in large-scale, real-world data so far. Methods: Leveraging data from the UK Biobank, encompassing 445,493 individuals aged 40-69, we examined associations of high 25-hydroxyvitamin (25(OH)D) levels ≥ 100 nmol/L and vitamin D supplementation with hypercalcemia (serum calcium > 2.6 mmol/L), kidney stones, and atherosclerosis assessments (pulse wave arterial stiffness index and carotid intima-medial thickness). Regression models were comprehensively adjusted for 49 covariates. Results: Approximately 1.5% of the participants had high 25(OH)D levels, 4.3% regularly used vitamin D supplements, and 20.4% reported regular multivitamin use. At baseline, the hypercalcemia prevalence was 1.6%, and 1.1% was diagnosed with kidney stones during follow-up. High 25(OH)D levels were neither associated with calcium-related adverse events nor atherosclerosis assessments. Vitamin D and multivitamin supplementation were associated with an increased prevalence of hypercalcemia (odds ratios and 95% confidence intervals: 1.46 [1.32-1.62] and 1.11 [1.04-1.18], respectively) but were neither associated with atherosclerosis nor future kidney stones. Conclusions: High 25(OH)D levels observable in routine care were not associated with any adverse outcome. Vitamin D users have a slightly higher prevalence of hypercalcemia, possibly due to co-supplementation with calcium, but without a higher atherosclerosis prevalence or risk of kidney stones.
Keywords: adverse events; atherosclerosis; hypercalcemia; kidney stone risk; real-world evidence; serum 25-hydroxyvitamin D levels; vitamin D supplementation.
Conflict of interest statement
All authors declare no conflicts of interest.
Figures
Similar articles
-
Association between serum 25-hydroxyvitamin D concentrations and kidney stone: a cohort study in the UK Biobank.Int Urol Nephrol. 2024 Nov;56(11):3585-3594. doi: 10.1007/s11255-024-04111-8. Epub 2024 Jun 6. Int Urol Nephrol. 2024. PMID: 38842659
-
Real-world evidence for an association of vitamin D supplementation with atherosclerotic cardiovascular disease in the UK Biobank.Clin Nutr. 2025 Jun;49:118-127. doi: 10.1016/j.clnu.2025.04.017. Epub 2025 Apr 16. Clin Nutr. 2025. PMID: 40267517
-
Monthly high-dose vitamin D supplementation does not increase kidney stone risk or serum calcium: results from a randomized controlled trial.Am J Clin Nutr. 2019 Jun 1;109(6):1578-1587. doi: 10.1093/ajcn/nqy378. Am J Clin Nutr. 2019. PMID: 31005969 Clinical Trial.
-
Adverse events from large dose vitamin D supplementation taken for one year or longer.J Steroid Biochem Mol Biol. 2019 Apr;188:29-37. doi: 10.1016/j.jsbmb.2018.12.002. Epub 2018 Dec 6. J Steroid Biochem Mol Biol. 2019. PMID: 30529281
-
Vitamin D, Hypercalciuria and Kidney Stones.Nutrients. 2018 Mar 17;10(3):366. doi: 10.3390/nu10030366. Nutrients. 2018. PMID: 29562593 Free PMC article. Review.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
