

Native Infective Endocarditis: A State-of-the-Art-Review
- PMID: 39065249
- PMCID: PMC11278776
- DOI: 10.3390/microorganisms12071481
Native Infective Endocarditis: A State-of-the-Art-Review
Abstract
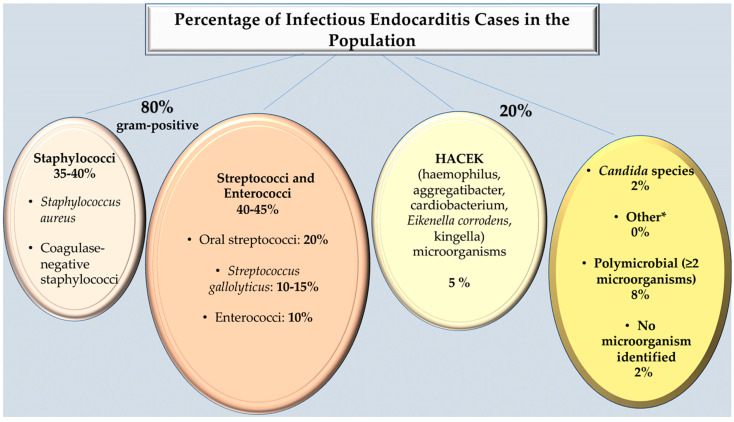
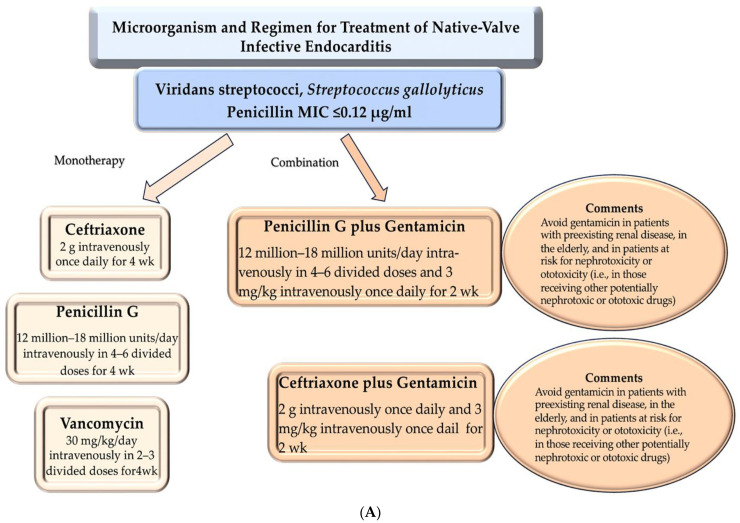
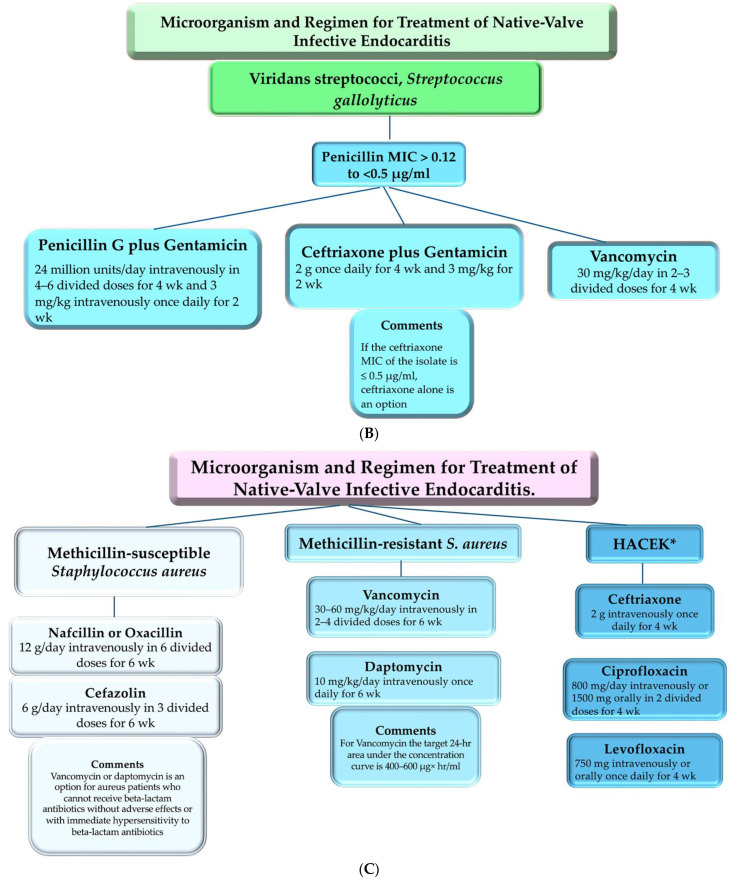
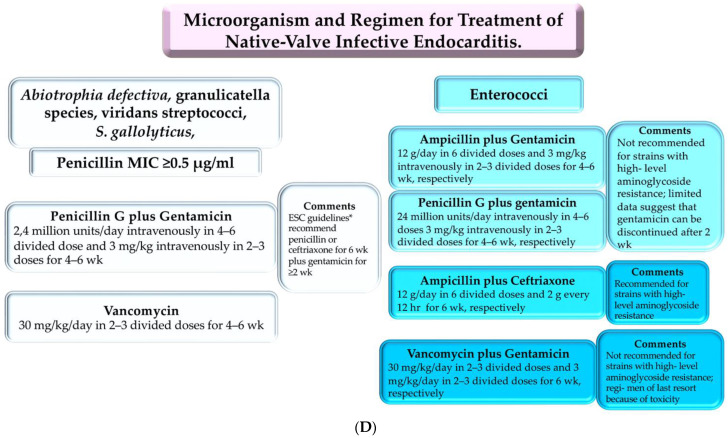
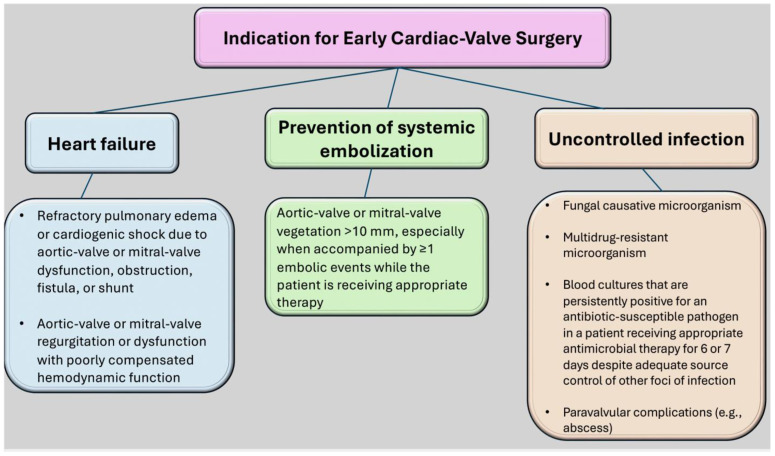
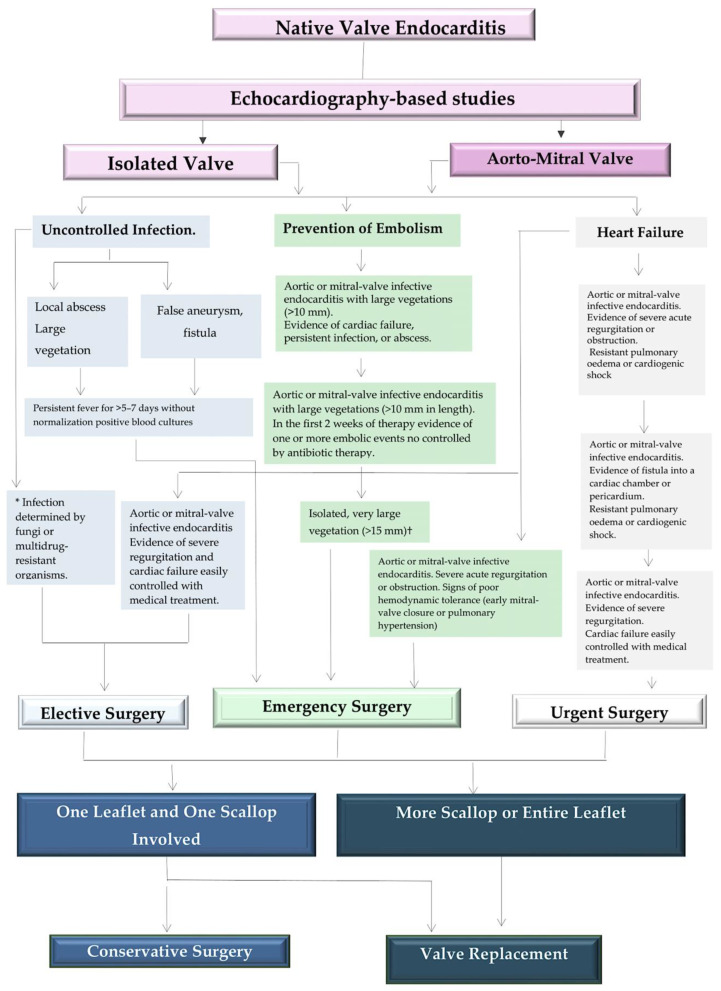
Native valve infective endocarditis (NVE) is a global phenomenon, defined by infection of a native heart valve and involving the endocardial surface. The causes and epidemiology of the disease have evolved in recent decades, with a doubling of the average patient age. A higher incidence was observed in patients with implanted cardiac devices that can result in right-sided infection of the tricuspid valve. The microbiology of the disease has also changed. Previously, staphylococci, which are most often associated with health-care contact and invasive procedures, were the most common cause of the disease. This has now been superseded by streptococci. While innovative diagnostic and therapeutic strategies have emerged, mortality rates have not improved and remain at 30%, which is higher than that for many cancer diagnoses. The lack of randomized trials and logistical constraints impede clinical management, and long-standing controversies such as the use of antibiotic prophylaxis persist. This state of the art review addresses clinical practice, controversies, and strategies to combat this potentially devastating disease. A multidisciplinary team will be established to provide care for patients with presumptive NVE. The composition of the team will include specialists in cardiology, cardiovascular surgery, and infectious disease. The prompt administration of combination antimicrobial therapy is essential for effective NVE treatment. Additionally, a meticulous evaluation of each patient is necessary in order to identify any indications for immediate valve surgery. With the intention of promoting a more comprehensive understanding of the procedural management of native infective endocarditis and to furnish clinicians with a reference, the current evidence for the utilization of distinct strategies for the diagnosis and treatment of NVE are presented.
Keywords: gram-positive bacteria; infective endocarditis; native valve endocarditis; vegetation.
Conflict of interest statement
The author declares no conflicts of interest.
Figures
Similar articles
-
Infective endocarditis.Lancet. 2016 Feb 27;387(10021):882-93. doi: 10.1016/S0140-6736(15)00067-7. Epub 2015 Sep 1. Lancet. 2016. PMID: 26341945 Review.
-
Endocarditis caused by Staphylococcus aureus: A reappraisal of the epidemiologic, clinical, and pathologic manifestations with analysis of factors determining outcome.Medicine (Baltimore). 2009 Jan;88(1):1-22. doi: 10.1097/MD.0b013e318194da65. Medicine (Baltimore). 2009. PMID: 19352296
-
Emergence of coagulase-negative staphylococci as a cause of native valve endocarditis.Clin Infect Dis. 2008 Jan 15;46(2):232-42. doi: 10.1086/524666. Clin Infect Dis. 2008. PMID: 18171255
-
Impact of a multidisciplinary management strategy on the outcome of patients with native valve infective endocarditis.Am J Cardiol. 2013 Oct 15;112(8):1171-6. doi: 10.1016/j.amjcard.2013.05.060. Epub 2013 Jul 5. Am J Cardiol. 2013. PMID: 23831163
-
Native and prosthetic valve infective endocarditis: clinicopathologic correlation and review of the literature.Malays J Pathol. 2014 Aug;36(2):71-81. Malays J Pathol. 2014. PMID: 25194529 Review.
Cited by
-
Infectious endocarditis complicated with intracranial infected aneurysm rupture and sinus of valsalva aneurysm rupture.BMC Neurol. 2024 Oct 4;24(1):372. doi: 10.1186/s12883-024-03870-2. BMC Neurol. 2024. PMID: 39367294 Free PMC article.
-
Advancements and Challenges in the Management of Prosthetic Valve Endocarditis: A Review.Pathogens. 2024 Nov 26;13(12):1039. doi: 10.3390/pathogens13121039. Pathogens. 2024. PMID: 39770299 Free PMC article. Review.
-
Etiological Aspects of Infectious Endocarditis in a Tertiary Hospital in Northeastern Romania.Medicina (Kaunas). 2025 Jan 9;61(1):95. doi: 10.3390/medicina61010095. Medicina (Kaunas). 2025. PMID: 39859077 Free PMC article.
-
Staphylococcus aureus in Inflammation and Pain: Update on Pathologic Mechanisms.Pathogens. 2025 Feb 12;14(2):185. doi: 10.3390/pathogens14020185. Pathogens. 2025. PMID: 40005560 Free PMC article. Review.
-
Trends of infective endocarditis mortality in young adult population of US: A concerning rise and its association with substance abuse.Int J Cardiol Cardiovasc Risk Prev. 2025 Apr 15;25:200404. doi: 10.1016/j.ijcrp.2025.200404. eCollection 2025 Jun. Int J Cardiol Cardiovasc Risk Prev. 2025. PMID: 40330157 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
