

Interventions to improve system-level coproduction in the Cystic Fibrosis Learning Network
- PMID: 39067867
- PMCID: PMC11287073
- DOI: 10.1136/bmjoq-2024-002860
Interventions to improve system-level coproduction in the Cystic Fibrosis Learning Network
Abstract
Background: Coproduction is defined as patients and clinicians collaborating equally and reciprocally in healthcare and is a crucial concept for quality improvement (QI) of health services. Learning Health Networks (LHNs) provide insights to integrate coproduction with QI efforts from programmes from various health systems.
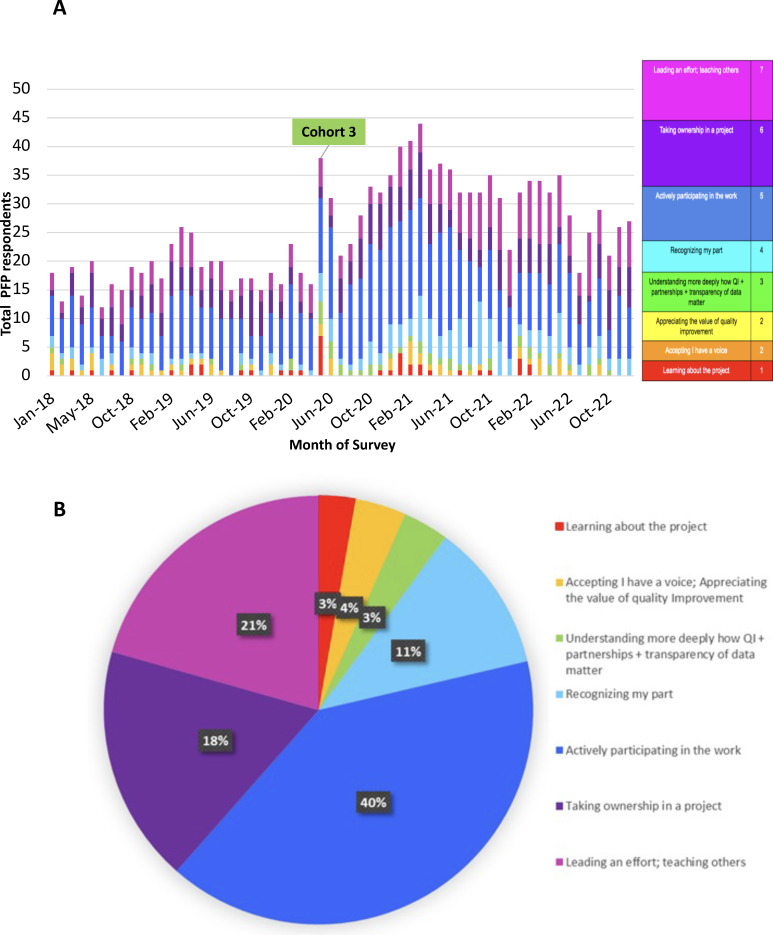
Objective: We describe interventions to develop and maintain patient and family partner (PFP) coproduction, measured by PFP-reported and programme-reported scales. We aim to increase percentage of programmes with PFPs reporting active QI work within their programme, while maintaining satisfaction in PFP-clinician relationships.
Methods: Conducted in the Cystic Fibrosis Learning Network (CFLN), an LHN comprising over 30 cystic fibrosis (CF) programmes, people with CF, caregivers and clinicians cocreated interventions in readiness awareness, inclusive PFP recruitment, onboarding process, partnership development and leadership opportunities. Interventions were adapted by CFLN programmes and summarised in a change package for existing programmes and the orientation of new ones. We collected monthly assessments for PFP and programme perceptions of coproduction and PFP self-rated competency of QI skills and satisfaction with programme QI efforts. We used control charts to analyse coproduction scales and run charts for PFP self-ratings.
Results: Between 2018 and 2022, the CFLN expanded to 34 programmes with 52% having ≥1 PFP reporting active QI participation. Clinicians from 76% of programmes reported PFPs were actively participating or leading QI efforts. PFPs reported increased QI skills competency (17%-32%) and consistently high satisfaction and feeling valued in their work.
Conclusions: Implementing system-level programmatic strategies to engage and sustain partnerships between clinicians and patients and families with CF improved perceptions of coproduction to conduct QI work. Key adaptable strategies for programmes included onboarding and QI training, supporting multiple PFPs simultaneously and developing financial recognition processes. Interventions may be applicable in other health conditions beyond CF seeking to foster the practice of coproduction.
Keywords: community-based participatory research; healthcare quality improvement; patient participation; patient-centred care; teamwork.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: KS is an employee of the Cystic Fibrosis Foundation and project officer for the SEID19AB0 grant award. DA is an Editorial Board Member of Therapeutic Advances in Respiratory Disease.
Figures



References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical