

Influence of virtual reality and task complexity on digital health metrics assessing upper limb function
- PMID: 39068424
- PMCID: PMC11282591
- DOI: 10.1186/s12984-024-01413-x
Influence of virtual reality and task complexity on digital health metrics assessing upper limb function
Abstract
Background: Technology-based assessments using 2D virtual reality (VR) environments and goal-directed instrumented tasks can deliver digital health metrics describing upper limb sensorimotor function that are expected to provide sensitive endpoints for clinical studies. Open questions remain about the influence of the VR environment and task complexity on such metrics and their clinimetric properties.
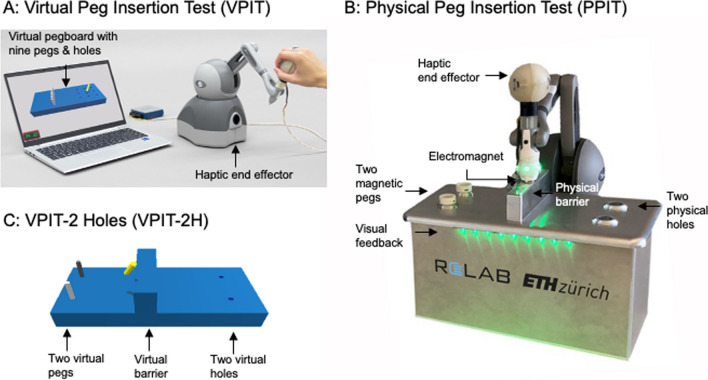
Methods: We aim to investigate the influence of VR and task complexity on the clinimetric properties of digital health metrics describing upper limb function. We relied on the Virtual Peg Insertion Test (VPIT), a haptic VR-based assessment with a virtual manipulation task. To evaluate the influence of VR and task complexity, we designed two novel tasks derived from the VPIT, the VPIT-2H (VR environment with reduced task complexity) and the PPIT (physical task with reduced task complexity). These were administered in an observational longitudinal study with 27 able-bodied participants and 31 participants with multiple sclerosis (pwMS, VPIT and PPIT only) and the value of kinematic and kinetic metrics, their clinimetric properties, and the usability of the assessment tasks were compared.
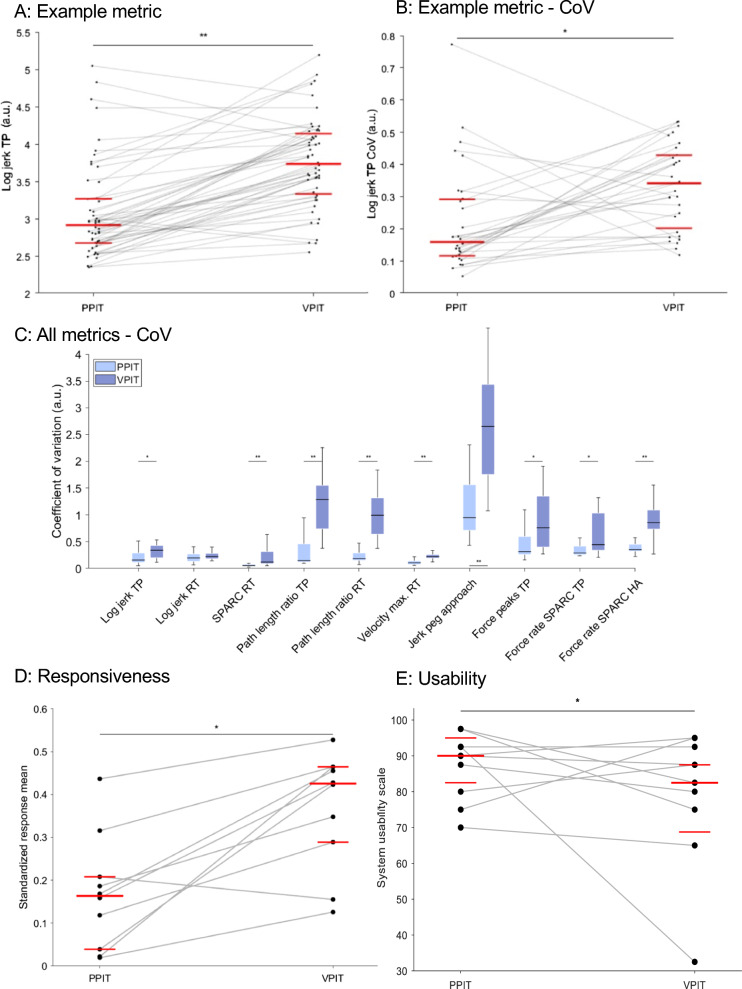
Results: Intra-participant variability strongly increased with increasing task complexity (coefficient of variation + 56%) and was higher in the VR compared to the physical environment (+ 27%). Surprisingly, this did not translate into significant differences in the metrics' measurement error and test-retest reliability across task conditions (p > 0.05). Responsiveness to longitudinal changes in pwMS was even significantly higher (effect size + 0.35, p < 0.05) for the VR task with high task complexity compared to the physical instrumented task with low task complexity. Increased inter-participant variability might have compensated for the increased intra-participant variability to maintain good clinimetric properties. No significant influence of task condition on concurrent validity was present in pwMS. Lastly, pwMS rated the PPIT with higher usability than the VPIT (System Usability Scale + 7.5, p < 0.05).
Conclusion: The metrics of both the VR haptic- and physical task-based instrumented assessments showed adequate clinimetric properties. The VR haptic-based assessment may be superior when longitudinally assessing pwMS due to its increased responsiveness. The physical instrumented task may be advantageous for regular clinical use due to its higher usability. These findings highlight that both assessments should be further validated for their ideal use-cases.
© 2024. The Author(s).
Conflict of interest statement
OL is a member of the Editorial Board of Journal of NeuroEngineering and Rehabilitation. OL was not involved in the journal’s peer review process of, or decisions related to, this manuscript. The authors do not have any other competing interests.
Figures


References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
