

Blood Biomarkers to Detect Alzheimer Disease in Primary Care and Secondary Care
- PMID: 39068545
- PMCID: PMC11284636
- DOI: 10.1001/jama.2024.13855
Blood Biomarkers to Detect Alzheimer Disease in Primary Care and Secondary Care
Abstract
Importance: An accurate blood test for Alzheimer disease (AD) could streamline the diagnostic workup and treatment of AD.
Objective: To prospectively evaluate a clinically available AD blood test in primary care and secondary care using predefined biomarker cutoff values.
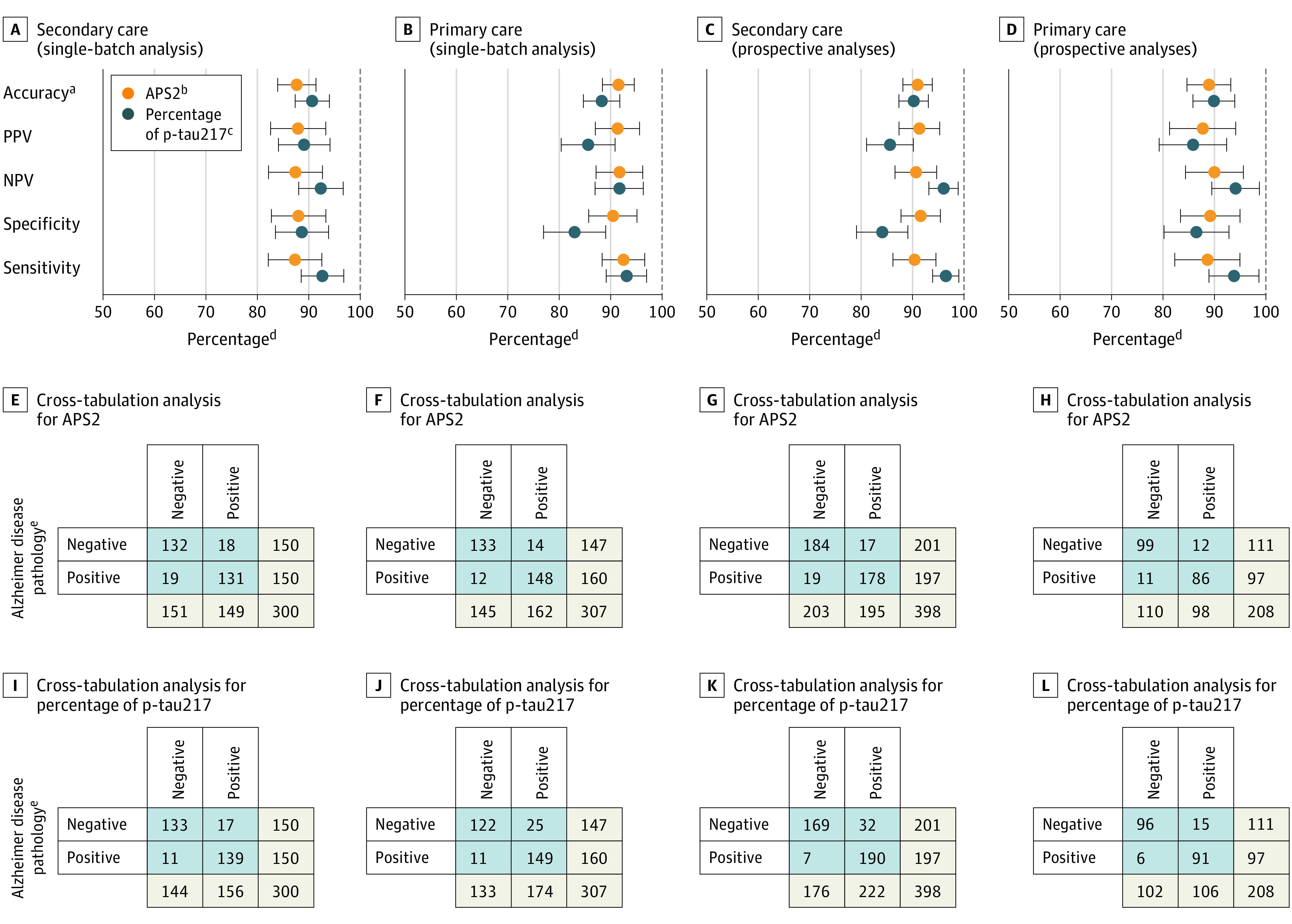
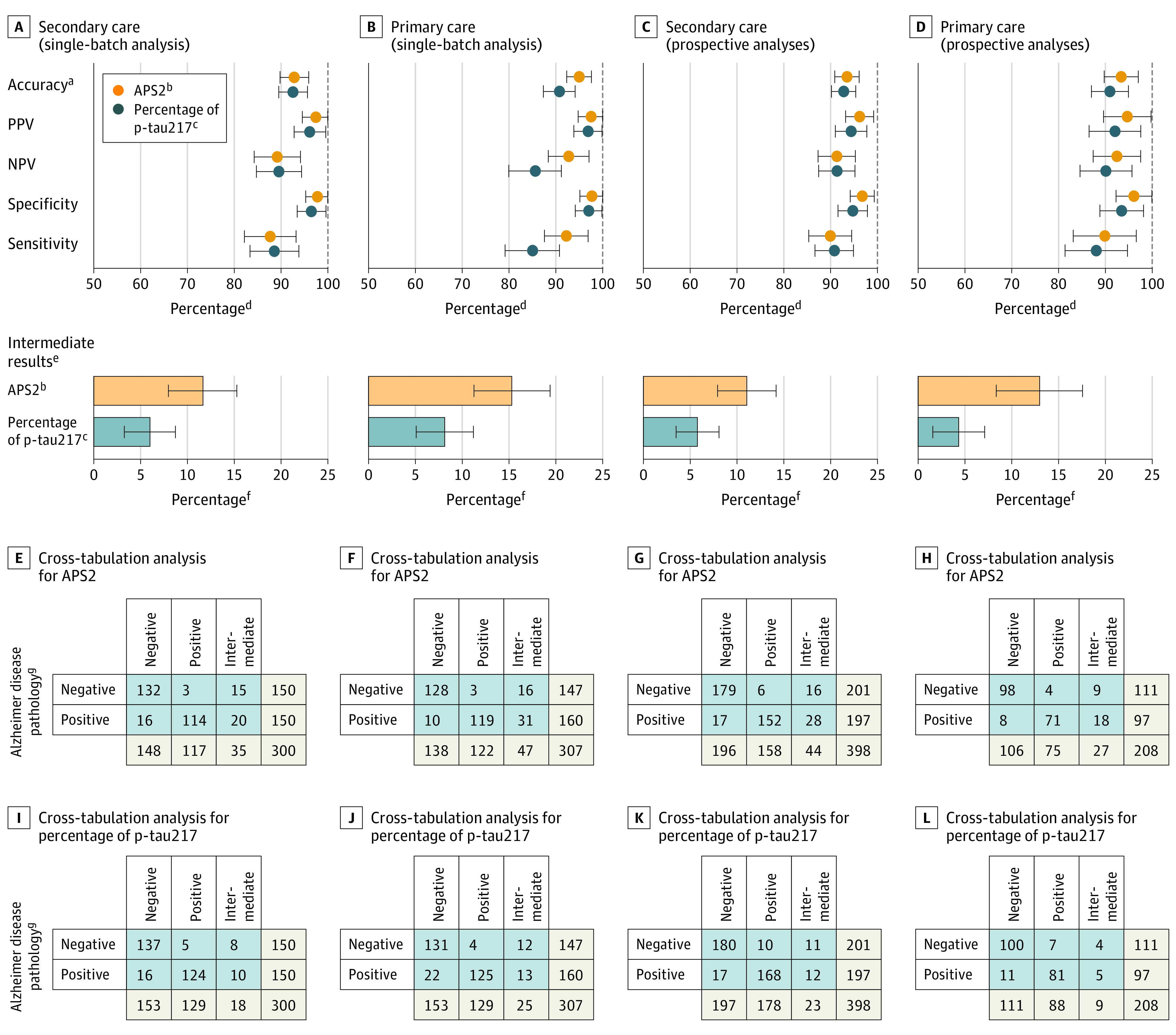
Design, setting, and participants: There were 1213 patients undergoing clinical evaluation due to cognitive symptoms who were examined between February 2020 and January 2024 in Sweden. The biomarker cutoff values had been established in an independent cohort and were applied to a primary care cohort (n = 307) and a secondary care cohort (n = 300); 1 plasma sample per patient was analyzed as part of a single batch for each cohort. The blood test was then evaluated prospectively in the primary care cohort (n = 208) and in the secondary care cohort (n = 398); 1 plasma sample per patient was sent for analysis within 2 weeks of collection.
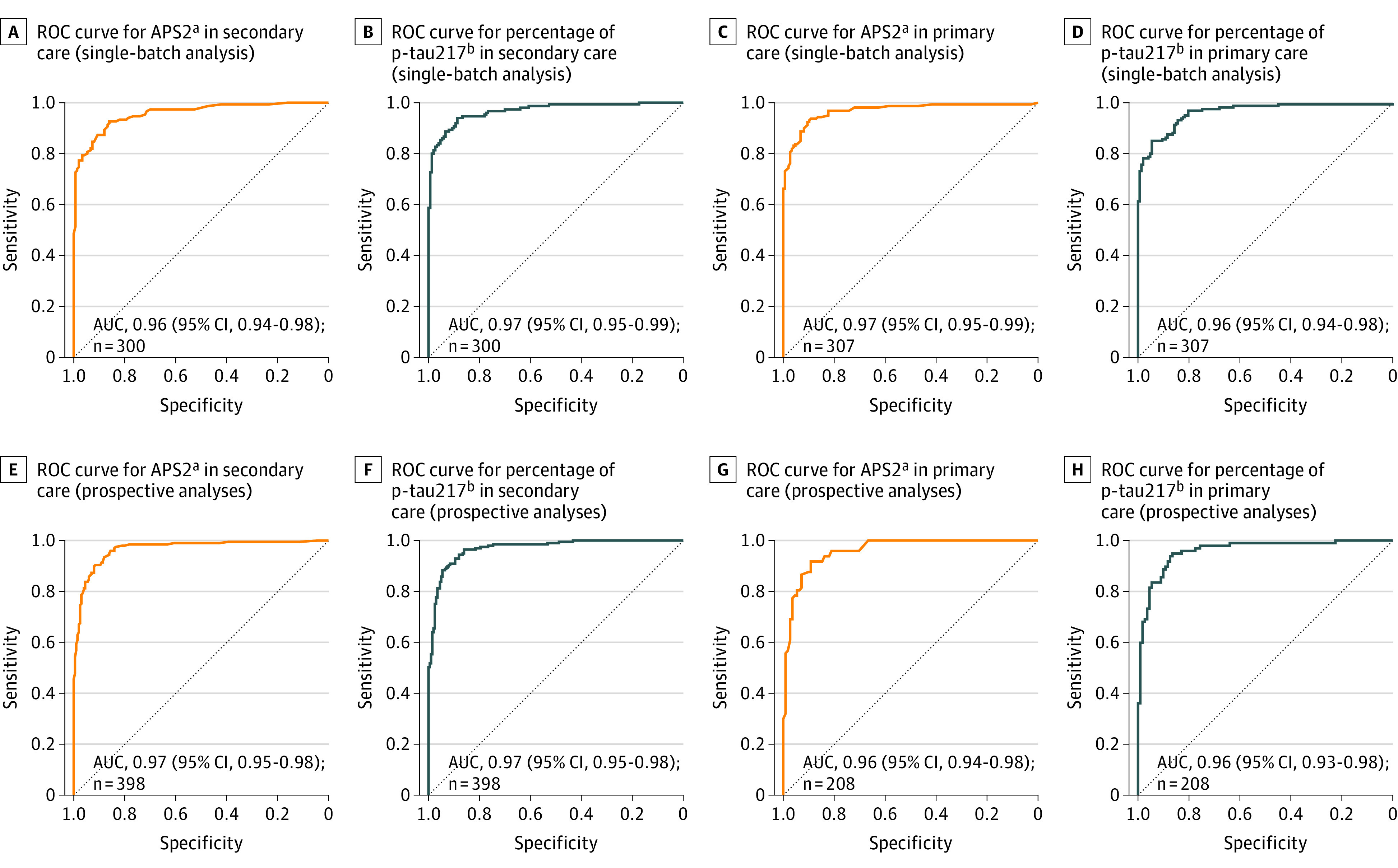
Exposure: Blood tests based on plasma analyses by mass spectrometry to determine the ratio of plasma phosphorylated tau 217 (p-tau217) to non-p-tau217 (expressed as percentage of p-tau217) alone and when combined with the amyloid-β 42 and amyloid-β 40 (Aβ42:Aβ40) plasma ratio (the amyloid probability score 2 [APS2]).
Main outcomes and measures: The primary outcome was AD pathology (determined by abnormal cerebrospinal fluid Aβ42:Aβ40 ratio and p-tau217). The secondary outcome was clinical AD. The positive predictive value (PPV), negative predictive value (NPV), diagnostic accuracy, and area under the curve (AUC) values were calculated.
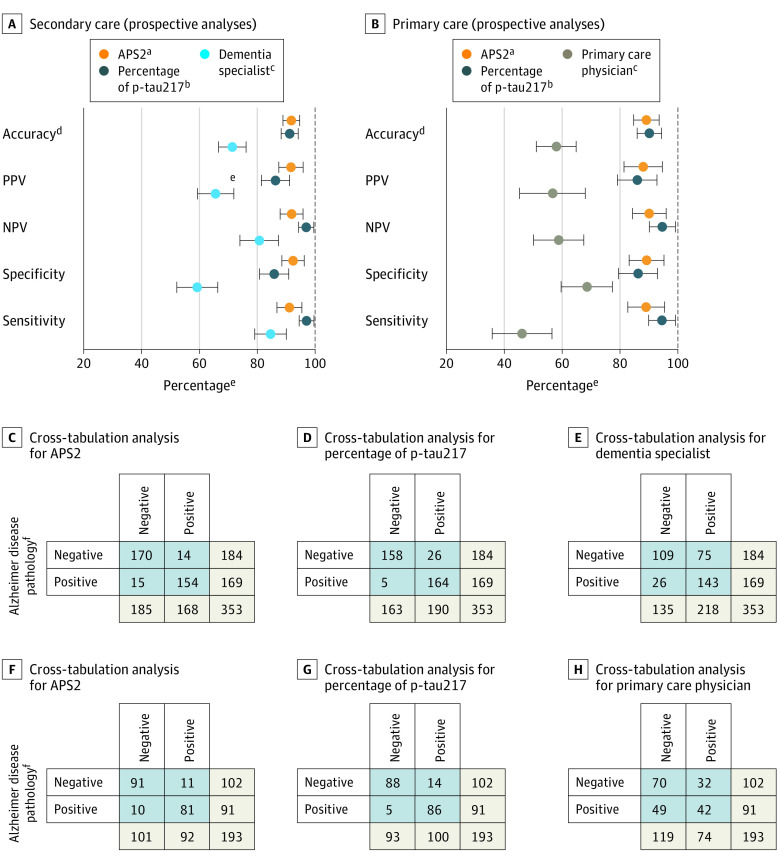
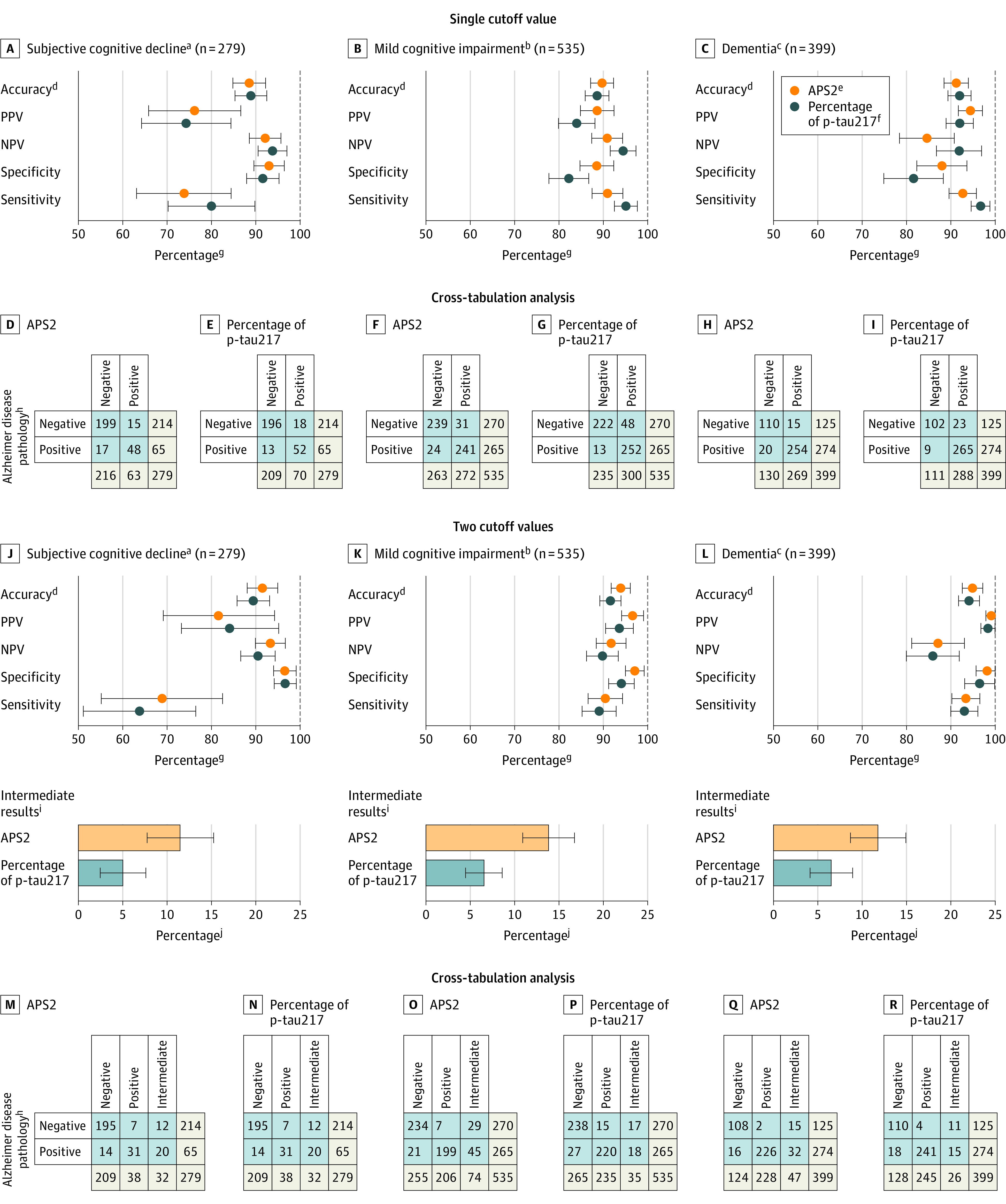
Results: The mean age was 74.2 years (SD, 8.3 years), 48% were women, 23% had subjective cognitive decline, 44% had mild cognitive impairment, and 33% had dementia. In both the primary care and secondary care assessments, 50% of patients had AD pathology. When the plasma samples were analyzed in a single batch in the primary care cohort, the AUC was 0.97 (95% CI, 0.95-0.99) when the APS2 was used, the PPV was 91% (95% CI, 87%-96%), and the NPV was 92% (95% CI, 87%-96%); in the secondary care cohort, the AUC was 0.96 (95% CI, 0.94-0.98) when the APS2 was used, the PPV was 88% (95% CI, 83%-93%), and the NPV was 87% (95% CI, 82%-93%). When the plasma samples were analyzed prospectively (biweekly) in the primary care cohort, the AUC was 0.96 (95% CI, 0.94-0.98) when the APS2 was used, the PPV was 88% (95% CI, 81%-94%), and the NPV was 90% (95% CI, 84%-96%); in the secondary care cohort, the AUC was 0.97 (95% CI, 0.95-0.98) when the APS2 was used, the PPV was 91% (95% CI, 87%-95%), and the NPV was 91% (95% CI, 87%-95%). The diagnostic accuracy was high in the 4 cohorts (range, 88%-92%). Primary care physicians had a diagnostic accuracy of 61% (95% CI, 53%-69%) for identifying clinical AD after clinical examination, cognitive testing, and a computed tomographic scan vs 91% (95% CI, 86%-96%) using the APS2. Dementia specialists had a diagnostic accuracy of 73% (95% CI, 68%-79%) vs 91% (95% CI, 88%-95%) using the APS2. In the overall population, the diagnostic accuracy using the APS2 (90% [95% CI, 88%-92%]) was not different from the diagnostic accuracy using the percentage of p-tau217 alone (90% [95% CI, 88%-91%]).
Conclusions and relevance: The APS2 and percentage of p-tau217 alone had high diagnostic accuracy for identifying AD among individuals with cognitive symptoms in primary and secondary care using predefined cutoff values. Future studies should evaluate how the use of blood tests for these biomarkers influences clinical care.
Conflict of interest statement
Figures
Comment in
-
Are Blood Tests for Alzheimer Disease Ready for Prime Time?JAMA. 2024 Oct 15;332(15):1240-1241. doi: 10.1001/jama.2024.12814. JAMA. 2024. PMID: 39068544 No abstract available.
-
Blood-Based Biomarkers for Alzheimer Disease-Ready for Primary Care?JAMA Neurol. 2024 Oct 1;81(10):1030-1031. doi: 10.1001/jamaneurol.2024.2801. JAMA Neurol. 2024. PMID: 39068546 No abstract available.
-
Alzheimer-Bluttest für die Hausarztpraxis.MMW Fortschr Med. 2025 Feb;167(2):30. doi: 10.1007/s15006-025-4674-4. MMW Fortschr Med. 2025. PMID: 39915399 Review. German. No abstract available.
References
-
- Alzheimer's Association . 2021 Alzheimer’s disease facts and figures. Alzheimers Dement. 2021;17(3):327-406. - PubMed
-
- Hansson O. Biomarkers for neurodegenerative diseases. Nat Med. 2021;27(6):954-963. - PubMed
-
- van Dyck CH, Swanson CJ, Aisen P, et al. Lecanemab in early Alzheimer’s disease. N Engl J Med. 2023;388(1):9-21. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
