

Surgical intervention for lung cancer in patients aged 75 and above: potential associations with increased mortality rates-a single-center observational study
- PMID: 39069611
- PMCID: PMC11285345
- DOI: 10.1186/s13019-024-02922-5
Surgical intervention for lung cancer in patients aged 75 and above: potential associations with increased mortality rates-a single-center observational study
Abstract
Background: Lung cancer, which is diagnosed two to three times more frequently in patients over the age of 70, is a leading cause of cancer-specific mortality. Given the elevated risk of morbidity and mortality, surgical intervention may not always be the most appropriate primary treatment option. This study aims to evaluate specific risk factors associated with postoperative morbidity and mortality in elderly patients and to optimize patient selection therefore improving surgical outcomes.
Patients and methods: The study encompassed a cohort of 73 patients aged 75 and above who underwent surgical treatment for non-small cell lung cancer (NSCLC) at the Department of Thoracic Surgery of the P. Hertsen Moscow Oncological Research Institute between 2015 and 2021. All patients underwent preoperative evaluation, including PET/CT staging and functional assessment, carried out by a multidisciplinary team comprising thoracic surgeons, anesthesiologists, and other medical specialists.
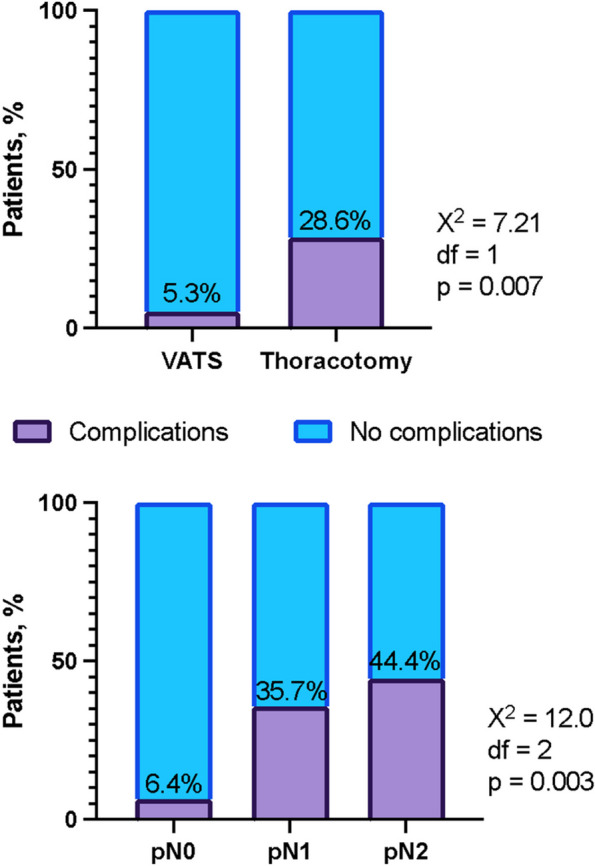
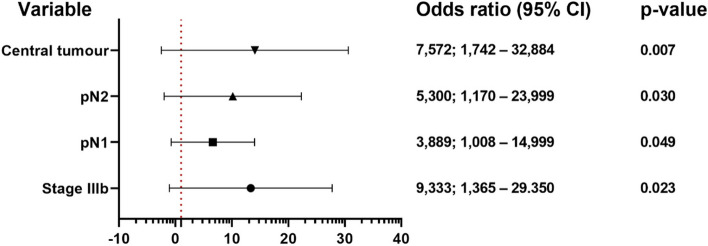
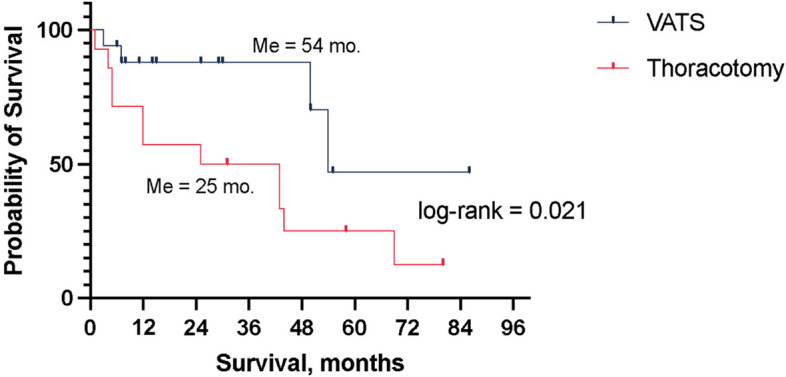
Results: The investigation revealed a postoperative mortality rate of 5.5% and a postoperative morbidity incidence of 16.4%, with occurrences of atrial fibrillation in 41.6%, persistent air leak in 33.3%, and pneumonia in 25% of complicated cases. At the one-year follow-up, 88% of patients remained free from relapse, whereas at three years, this rate stood at 66%. During the follow-up period, 16 patients (22%) passed away, with a median survival duration of 44 months. Survival rates at one year, three years, and five years were 71%, 66%, and 35%, respectively. Multivariate analysis disclosed several significant factors predicting a complex postoperative period, including stage IIIb (p = 0.023), pN1 (p = 0.049), pN2 (p = 0.030), and central location (p = 0.007). Additionally, overall survival was primarily influenced by a Charlson comorbidity index of 6 (p = 0.044), stage Ia2 (p = 0.033), and the necessity for thoracotomy (p = 0.045).
Conclusion: Each case of lung cancer in patients aged 75 and older necessitates an individualized approach. Given the higher mortality rate relative to younger patients, comprehensive risk assessment and preoperative management of underlying comorbidities are imperative, with the involvement of anesthesiologists, intensive care physicians, cardiologists, and other relevant specialists as needed.
Keywords: Complications; Elderly; Perioperative period; Pulmonary surgical procedure.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- He W, Goodkind D, Kowal PR. An aging world: 2015. Washington, DC: U.S. Government Publishing Office; 2016.
-
- Okami J, Higashiyama M, Asamura H, et al. Pulmonary resection in patients aged 80 years or over with clinical stage I non-small cell lung cancer: prognostic factors for overall survival and risk factors for postoperative complications. J Thorac Oncol. 2009;4(10):1247–53. 10.1097/JTO.0b013e3181ae285d. 10.1097/JTO.0b013e3181ae285d - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
