

The presence of circulating human apolipoprotein J reduces the occurrence of cerebral microbleeds in a transgenic mouse model with cerebral amyloid angiopathy
- PMID: 39069622
- PMCID: PMC11285315
- DOI: 10.1186/s13195-024-01541-5
The presence of circulating human apolipoprotein J reduces the occurrence of cerebral microbleeds in a transgenic mouse model with cerebral amyloid angiopathy
Abstract
Background: Cerebral amyloid angiopathy (CAA) is characterized by amyloid-β (Aβ) deposition in cerebral vessels, leading to lobar cerebral microbleeds (CMB) and intracerebral hemorrhages (ICH). Apolipoprotein J (ApoJ) is a multifunctional chaperone related to Aβ aggregation and clearance. Our study investigated the vascular impact of chronic recombinant human Apolipoprotein J (rhApoJ) treatment in a transgenic mouse model of β-amyloidosis with prominent CAA.
Methods: Twenty-month-old APP23 C57BL/6 mice received 25 doses of rhApoJ (1 mg/kg) (n = 9) or saline (n = 8) intraperitoneally for 13 weeks, while Wild-type (WT) mice received saline (n = 13). Postmortem brains underwent T2*-weighted magnetic resonance imaging (MRI) to detect hemorrhagic lesions. Aβ levels and distribution, cerebral fibrinogen leakage, brain smooth muscle actin (sma), and plasma matrix metalloproteinases and inflammatory markers were analyzed after treatments. Additionally, plasma samples from 22 patients with lobar ICH were examined to determine the clinical relevance of the preclinical findings.
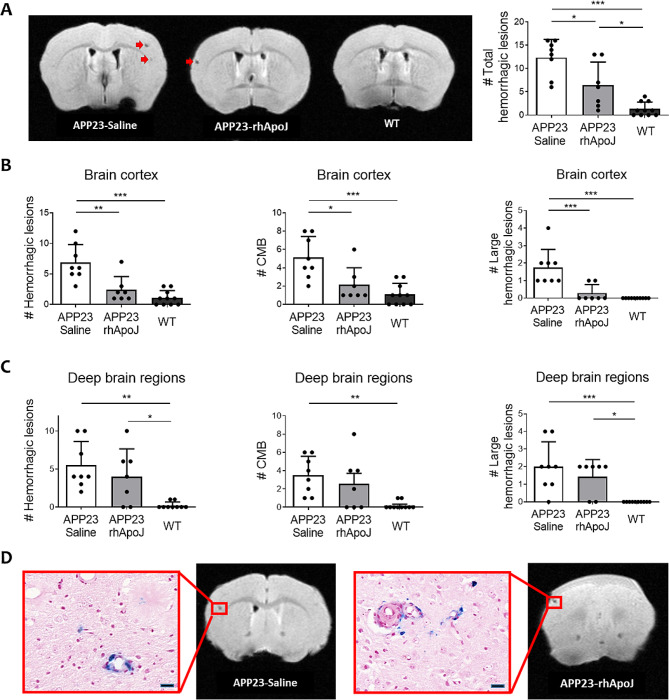
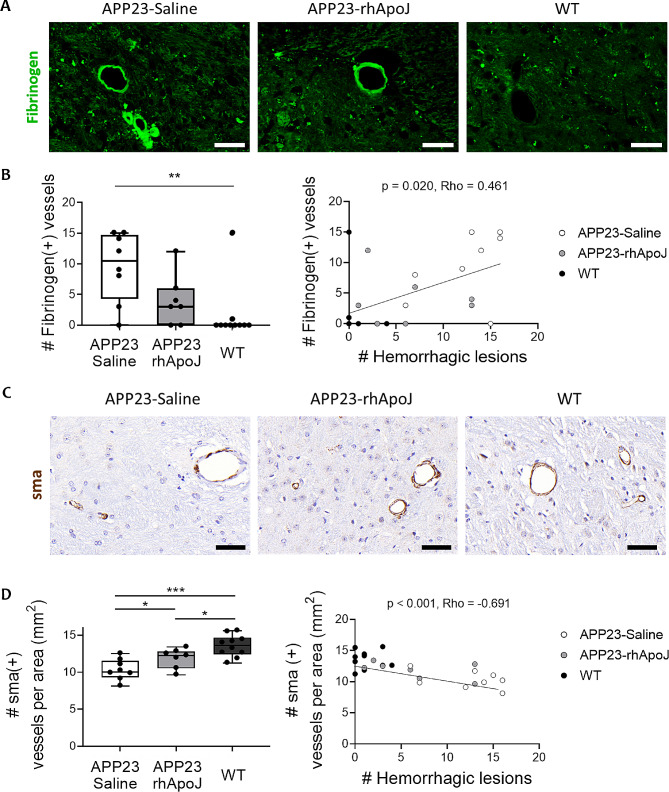
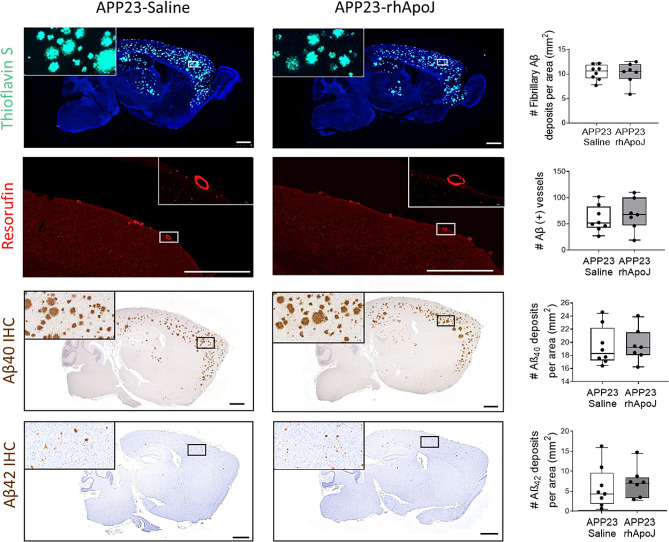
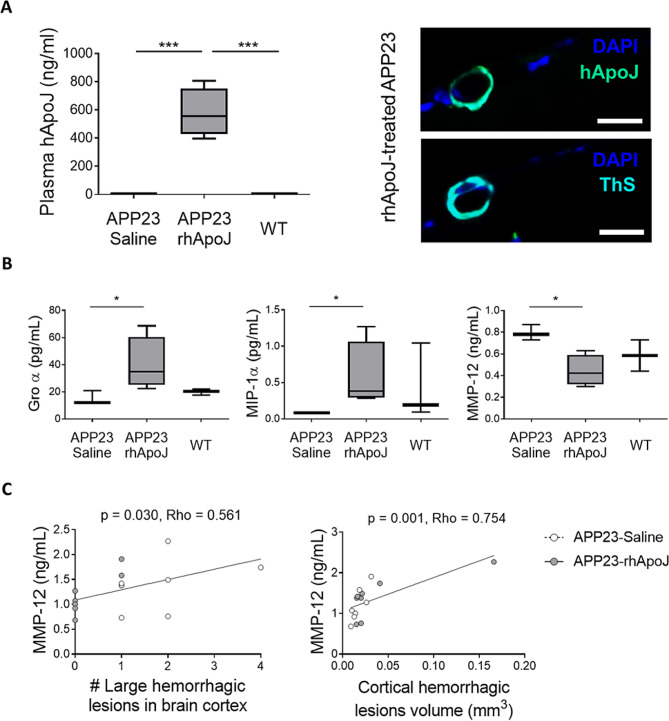
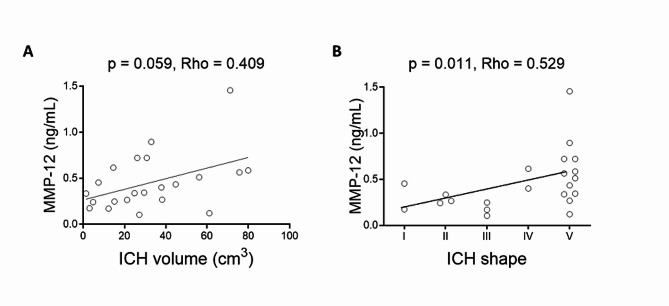
Results: rhApoJ-treated APP23 presented fewer cortical CMBs (50-300 μm diameter) (p = 0.012) and cortical larger hemorrhages (> 300 μm) (p = 0.002) than saline-treated mice, independently of Aβ brain levels. MRI-detected hemorrhagic lesions correlated with fibrinogen cerebral extravasation (p = 0.011). Additionally, rhApoJ-treated mice presented higher number of sma-positive vessels than saline-treated mice (p = 0.038). In rhApoJ-treated mice, human ApoJ was detected in plasma and in occasional leptomeningeal vessels, but not in the parenchyma, suggesting that its mechanism of action operates through the periphery. The administration of rhApoJ induced an increase in plasma Groα (p = 0.035) and MIP-1α (p = 0.035) levels, while lower MMP-12 (p = 0.046) levels, compared to the saline-treated group. In acute lobar ICH patients, MMP-12 plasma levels correlated with larger hemorrhage volume (p = 0.040) and irregular ICH shape (p = 0.036).
Conclusions: Chronic rhApoJ treatment in aged APP23 mice ameliorated CAA-related neurovascular damage by reducing the occurrence of CMB. We propose that rhApoJ may prevent blood-brain barrier (BBB) leakage and CMB appearance partly through circulating MMP-12 modulation.
Keywords: Amyloid-β; Apolipoprotein J; Cerebral amyloid Angiopathy; Cerebral microbleeds; MMP-12.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Charidimou A, Boulouis G, Frosch MP, Baron JC, Pasi M, Albucher JF, et al. The Boston criteria version 2.0 for cerebral amyloid angiopathy: a multicentre, retrospective, MRI-neuropathology diagnostic accuracy study. Lancet Neurol. 2022;21(8):714–25. 10.1016/S1474-4422(22)00208-3 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
- PI17/00275/Instituto de Salud Carlos III (ISCIII)
- PI17/00275/Instituto de Salud Carlos III (ISCIII)
- PI17/00275/Instituto de Salud Carlos III (ISCIII)
- PI17/00275/Instituto de Salud Carlos III (ISCIII)
- PI17/00275/Instituto de Salud Carlos III (ISCIII)
- PI17/00275/Instituto de Salud Carlos III (ISCIII)
- PI17/00275/Instituto de Salud Carlos III (ISCIII)
- PI17/00275/Instituto de Salud Carlos III (ISCIII)
- PI17/00275/Instituto de Salud Carlos III (ISCIII)
- RD21/0006/0007/RICORS-ICTUS-Enfermedades Vasculares Cerebrales network funded by ISCIII
- RD21/0006/0007/RICORS-ICTUS-Enfermedades Vasculares Cerebrales network funded by ISCIII
- RD21/0006/0007/RICORS-ICTUS-Enfermedades Vasculares Cerebrales network funded by ISCIII
- RD21/0006/0007/RICORS-ICTUS-Enfermedades Vasculares Cerebrales network funded by ISCIII
- RD21/0006/0007/RICORS-ICTUS-Enfermedades Vasculares Cerebrales network funded by ISCIII
- RD21/0006/0007/RICORS-ICTUS-Enfermedades Vasculares Cerebrales network funded by ISCIII
- RD21/0006/0007/RICORS-ICTUS-Enfermedades Vasculares Cerebrales network funded by ISCIII
- RD21/0006/0007/RICORS-ICTUS-Enfermedades Vasculares Cerebrales network funded by ISCIII
- RD21/0006/0007/RICORS-ICTUS-Enfermedades Vasculares Cerebrales network funded by ISCIII
- SGR2021/0656/Agència de Gestió d'Ajuts Universitaris i de Recerca
- SGR2021/0656/Agència de Gestió d'Ajuts Universitaris i de Recerca
- SGR2021/0656/Agència de Gestió d'Ajuts Universitaris i de Recerca
- SGR2021/0656/Agència de Gestió d'Ajuts Universitaris i de Recerca
- SGR2021/0656/Agència de Gestió d'Ajuts Universitaris i de Recerca
- SGR2021/0656/Agència de Gestió d'Ajuts Universitaris i de Recerca
- SGR2021/0656/Agència de Gestió d'Ajuts Universitaris i de Recerca
- SGR2021/0656/Agència de Gestió d'Ajuts Universitaris i de Recerca
- SGR2021/0656/Agència de Gestió d'Ajuts Universitaris i de Recerca
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
