

Primary SARS-CoV-2 infection in children and adults results in similar Fc-mediated antibody effector function patterns
- PMID: 39071109
- PMCID: PMC11273100
- DOI: 10.1002/cti2.1521
Primary SARS-CoV-2 infection in children and adults results in similar Fc-mediated antibody effector function patterns
Abstract
Objectives: Increasing evidence suggests that Fc-mediated antibody effector functions have an important role in protection against respiratory viruses, including SARS-CoV-2. However, limited data are available on the potential differences in the development, heterogeneity and durability of these responses in children compared to adults.
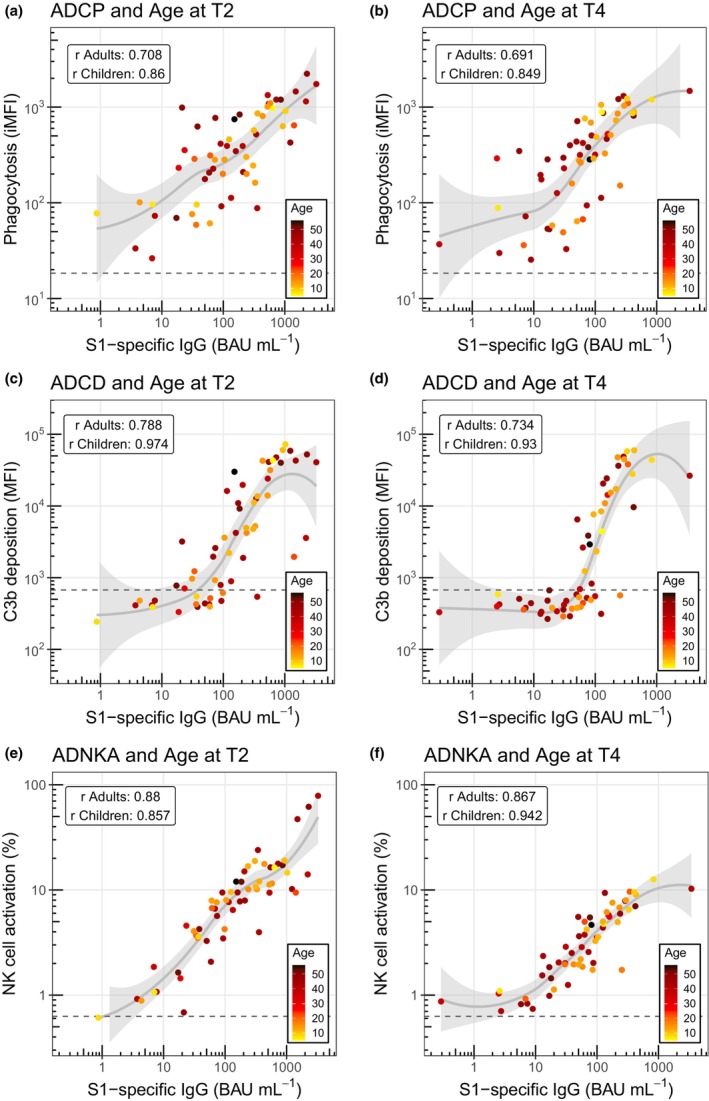
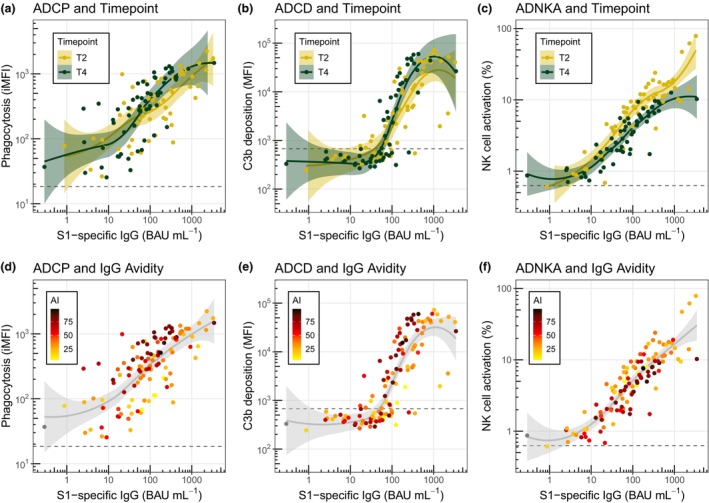
Methods: Here, we assessed the development of spike S1-specific serum antibody-dependent cellular phagocytosis (ADCP), complement deposition (ADCD) and natural killer cell activation (ADNKA), alongside specific antibody binding concentrations (IgG, IgA and IgM) and IgG avidity in healthy adults (n = 38, 18-56 years) and children (n = 21, 5-16 years) following primary SARS-CoV-2 infection, with a 10-month longitudinal follow-up. Differences between groups were assessed using a nonparametric Kruskal-Wallis test with Dunn's multiple comparisons test.
Results: We found similar (functional) antibody responses in children compared to adults, with a tendency for increased durability in children, which was statistically significant for ADCD (P < 0.05). While ADNKA was strongly reduced in both adults (P < 0.001) and children (P < 0.05) at the latest time point, ADCP remained relatively stable over time, possibly relating to an increase in avidity of the spike-specific antibodies (P < 0.001). Finally, the ADNKA capacity relative to antibody concentration appeared to decrease over time in both children and adults.
Conclusion: In conclusion, our data provide novel insights into the development of SARS-CoV-2-specific antibody Fc-mediated effector functions in children and adults. An increased understanding of these characteristics in specific age populations is valuable for the future design of novel and improved vaccination strategies for respiratory viruses such as SARS-CoV-2.
Keywords: Fc‐functionality; adults; children; monocytes; natural killer cells; viral infection.
© 2024 The Author(s). Clinical & Translational Immunology published by John Wiley & Sons Australia, Ltd on behalf of Australian and New Zealand Society for Immunology, Inc.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
LinkOut - more resources
Full Text Sources
Miscellaneous