

Supra-Alveolar Bone Regeneration: Progress, Challenges, and Future Perspectives
- PMID: 39071449
- PMCID: PMC11270636
- DOI: 10.1016/j.compositesb.2024.111673
Supra-Alveolar Bone Regeneration: Progress, Challenges, and Future Perspectives
Abstract
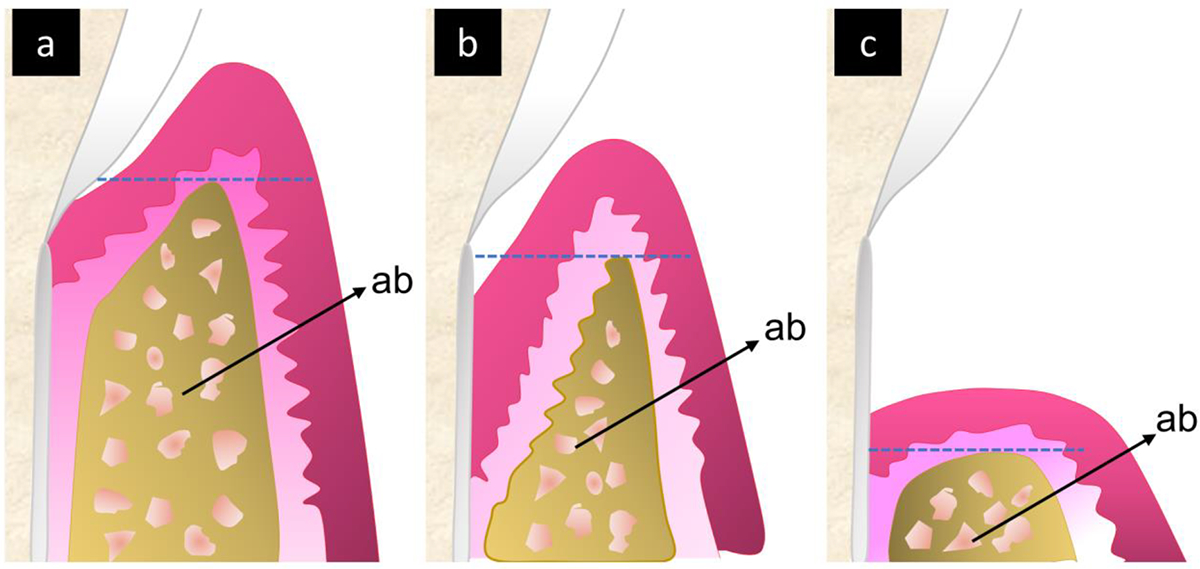
Periodontitis is a highly prevalent disease that damages the supporting tissues of a tooth, including the alveolar bone. Alveolar bone loss owing to periodontitis is broadly categorized as supra-alveolar and intra-alveolar bone loss. In intra-alveolar bone loss, the defect has an angular or oblique orientation to the long axis of the tooth in an apical direction. In contrast, the defect is perpendicular to the long axis of the tooth in supra-alveolar bone loss. Unlike intra-alveolar bone defects, supra-alveolar bone defects lack supporting adjacent space, which makes supra-alveolar bone regeneration more challenging. In addition, the limited availability of resources in terms of vascularity and underlying tissues is another obstacle to supra-alveolar bone regeneration. Currently, supra-alveolar bone loss is the least predictable periodontal defect type in regenerative periodontal therapy. In addition, supra-alveolar bone loss is much more common than other alveolar bone loss. Despite its prevalence, research on supra-alveolar bone regeneration remains sparse, indicating an unmet need for significant research efforts in this area. This review summarize recent advances, obstacles, and future directions in the field of supra-alveolar bone regeneration. We discuss the biomaterials, bioactive molecules, and cells that have been tested for supra-alveolar bone regeneration, followed by pre-clinical and clinical approaches employed in this field. Additionally, we highlight obstacles and present future directions that will propel supra-alveolar bone research forward.
Keywords: alveolar bone loss; dental materials; periodontitis; supra-alveolar bone; tissue regeneration.
Conflict of interest statement
Declaration of competing interest The authors declare that they do not have any competing financial or personal interests that could influence the work reported in this paper. Declaration of interests The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures

Similar articles
-
Recent advances in horizontal alveolar bone regeneration.Biomed Mater. 2023 Jul 24;18(5). doi: 10.1088/1748-605X/acd672. Biomed Mater. 2023. PMID: 37196651 Review.
-
Supra-Alveolar Periodontal Tissue Reconstruction in a Case with Severe Periodontitis: Case Report with a 2-Year Follow-up.Int J Periodontics Restorative Dent. 2023 Mar, Apr;43(2):212-221. doi: 10.11607/prd.6241. Int J Periodontics Restorative Dent. 2023. PMID: 37232683
-
Prognostic factors for alveolar regeneration: bone formation at teeth and titanium implants.J Clin Periodontol. 2004 Nov;31(11):927-32. doi: 10.1111/j.1600-051X.2004.00590.x. J Clin Periodontol. 2004. PMID: 15491305
-
Effect of allogeneic, freeze-dried, demineralized bone matrix on guided bone regeneration in supra-alveolar peri-implant defects in dogs.Int J Oral Maxillofac Implants. 1997 Sep-Oct;12(5):634-42. Int J Oral Maxillofac Implants. 1997. PMID: 9337024
-
Regenerative Medicine for Periodontal and Peri-implant Diseases.J Dent Res. 2016 Mar;95(3):255-66. doi: 10.1177/0022034515618887. Epub 2015 Nov 25. J Dent Res. 2016. PMID: 26608580 Free PMC article. Review.
Cited by
-
An axolotl limb regeneration-inspired strategy to enhance alveolar bone regeneration.Bioact Mater. 2025 Feb 19;48:242-256. doi: 10.1016/j.bioactmat.2025.02.020. eCollection 2025 Jun. Bioact Mater. 2025. PMID: 40046012 Free PMC article.
-
Injectable bioactive scaffold able to stimulate oral bone regeneration on demand.J Mater Sci Mater Med. 2025 Apr 8;36(1):31. doi: 10.1007/s10856-025-06879-2. J Mater Sci Mater Med. 2025. PMID: 40198381 Free PMC article.
-
Amorphous calcium zinc phosphate promotes macrophage-driven alveolar bone regeneration via modulation of energy metabolism and mitochondrial homeostasis.Bioact Mater. 2025 Jul 1;52:829-844. doi: 10.1016/j.bioactmat.2025.06.053. eCollection 2025 Oct. Bioact Mater. 2025. PMID: 40677756 Free PMC article.
-
Nanozymes Empower Periodontitis Treatment: New Strategies and Clinical Application Prospects.Biomater Res. 2025 May 20;29:0210. doi: 10.34133/bmr.0210. eCollection 2025. Biomater Res. 2025. PMID: 40395276 Free PMC article. Review.
References
-
- Papapanou PN, Tonetti MS. Diagnosis and epidemiology of periodontal osseous lesions. Periodontology 2000. 2000;22:8–21. - PubMed
-
- Greenstein B, Frantz B, Desai R, Proskin H, Campbell J, Caton J. Stability of treated angular and horizontal bony defects: a retrospective radiographic evaluation in a private periodontal practice. Journal of Periodontology. 2009;80(2):228–33. - PubMed
-
- Hansen BF, Gjermo P, Bergwitz-Larsen KR. Periodontal bone loss in 15-year-old Norwegians. Journal of Clinical Periodontology. 1984;11(2):125–31. - PubMed