

Microsurgical and endovascular treatment of large and giant aneurysms of the anterior circulation: A systematic review
- PMID: 39071454
- PMCID: PMC11279635
- DOI: 10.1016/j.bas.2024.102838
Microsurgical and endovascular treatment of large and giant aneurysms of the anterior circulation: A systematic review
Abstract
Introduction: Large and Giant intracranial aneurysms (LGIAs) have become the paradigm for which endovascular techniques do not provide satisfactory results. Yet, microsurgery is followed by non-negligible rates of morbimortality. This scenario may have changed since the introduction of flow-diversion devices.
Research question: Contemporary and standardised revision on microsurgical and endovascular results, with emphasis on anterior circulation LGIAs.
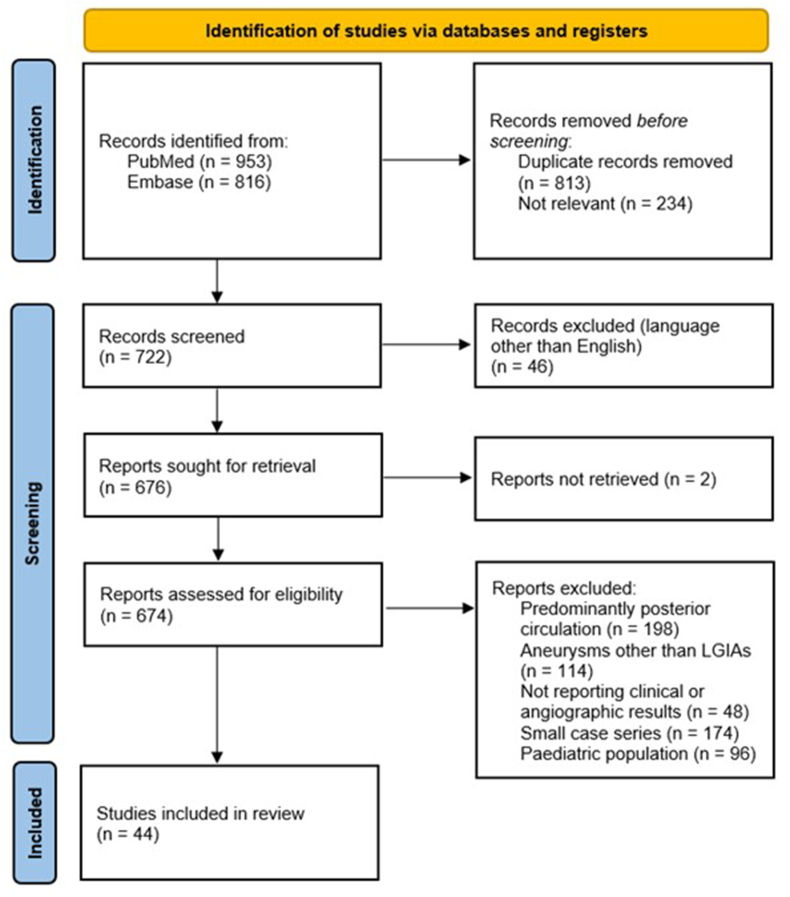
Materials and methods: A systematic literature search was conducted in two databases (PubMed and Embase) on treatment outcomes of LGIAs of the anterior circulation, after the introduction of flow-diverters 2008/01/01, till 2023/05/20. Small case series (<5 cases), series including >15% of posterior circulation aneurysms, and studies not reporting clinical and/or angiographic outcomes were excluded.
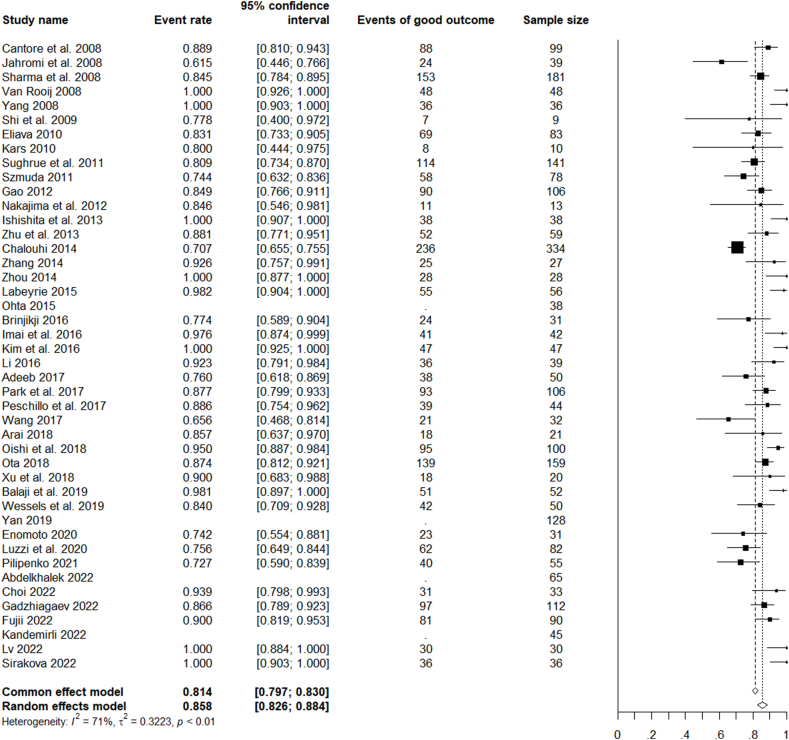
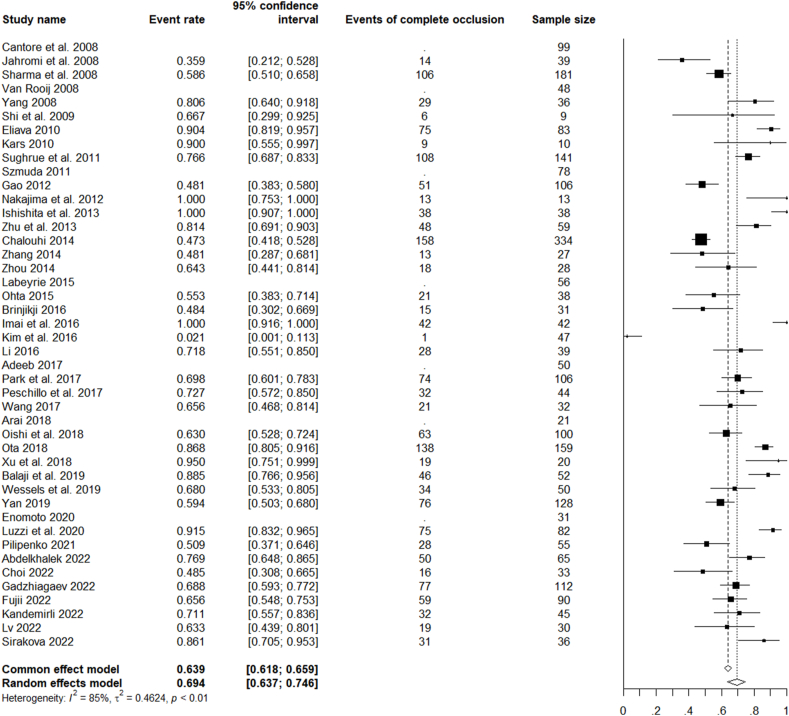
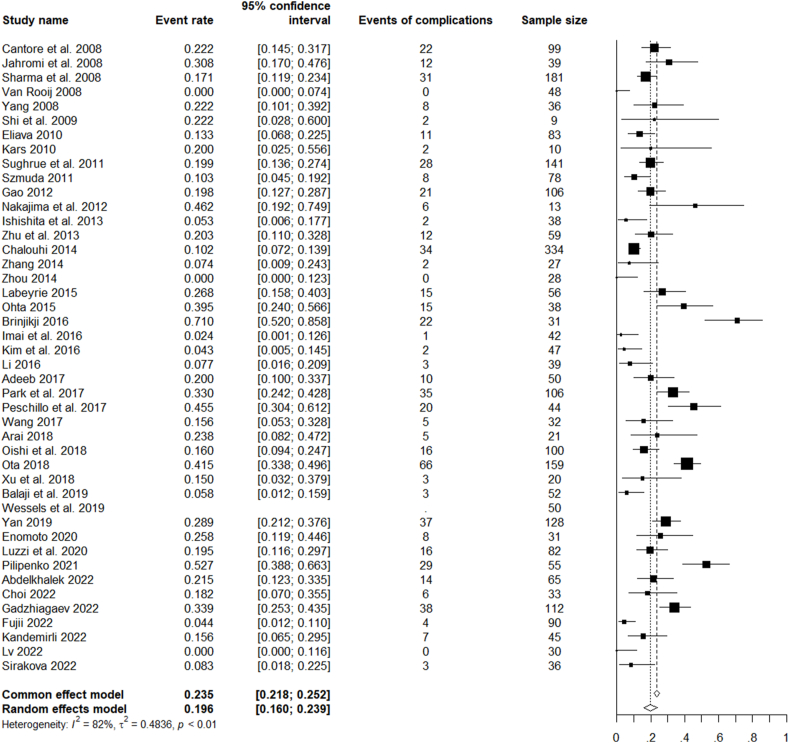
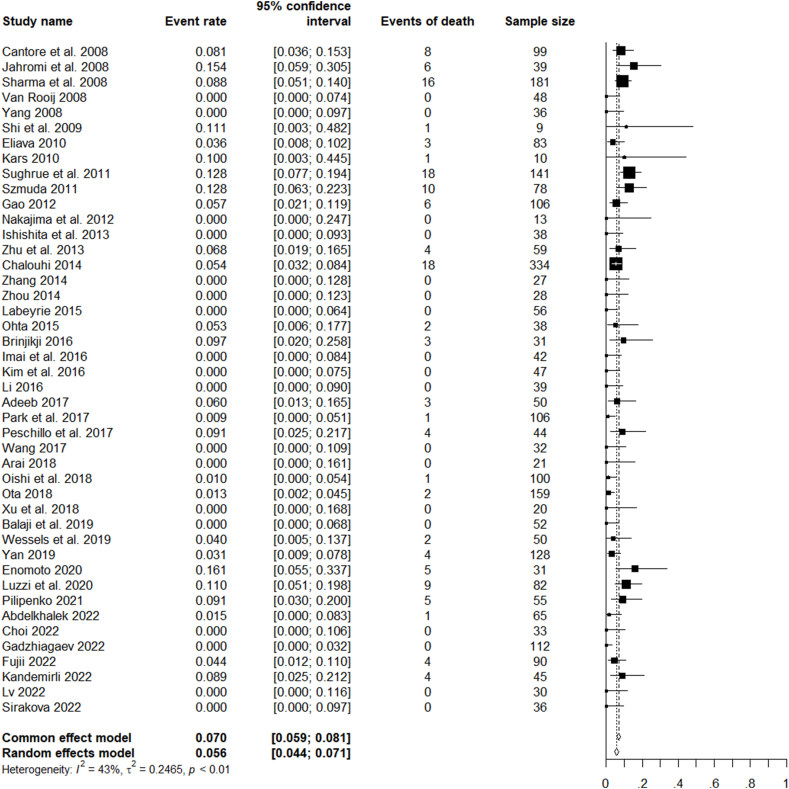
Results: 44 relevant studies (observational cohorts) were identified, including 2923 LGIAs predominantly from anterior circulation. Mean follow-up 22 (±20) months. 1494 (51%) LGIAs were treated endovascularly and 1427 (49%) microsurgically. According to the random effects model, pooled rates of favourable clinical outcomes were 85.8% (CI 95% 82.6-88.4), complete occlusion 69.4% (CI 95% 63.7-7.46), complications 19.6% (CI 95%16-23.9) and mortality 5.6% (CI 95% 4.4-7.1). Focusing on type of treatment, occlusion rates are higher with microsurgical (842/993, 85% vs 874/1,299, 67%), although good outcomes are slightly more frequent with endovascular (1045/1,135, 92% vs 1120/1,294, 87%).
Discussion and conclusions: According to contemporary data about occlusion rates, functional outcomes, and complications, primary or secondary treatment of LGIAs of the anterior circulation seems justified. Microsurgical occlusion rates are higher in LGIAs. An expert consensus on reporting complications and management strategies is warranted.
Keywords: Clip; Complete occlusion; Endovascular; Flow-diverter; Large giant intracranial aneurysms; Mortality; Surgery; Trap.
© 2024 The Authors.
Conflict of interest statement
The authors have no conflicts of interest regarding this article.
Figures
References
-
- Adeeb N., Griessenauer C.J., Shallwani H., Shakir H., Foreman P.M., Moore J.M., et al. Pipeline embolization device in treatment of 50 unruptured large and giant aneurysms. World Neurosurg. 2017;105:232–237. - PubMed
-
- Arai S., Mizutani T., Sugiyama T., Sumi K., Nakajo T., Matsumoto M., et al. Is surgical parent artery occlusion effective for intracranial aneurysms measuring over 10 mm in size? Result from long-term follow-up of size changes and outcomes. Acta Neurochir. 2019;161(1):185–195. - PubMed
-
- Barrow D.L., Alleyne C. Natural history of giant intracranial aneurysms and indications for intervention. Clin. Neurosurg. 1995;42:214–244. - PubMed
LinkOut - more resources
Full Text Sources
