

This is a preprint.
Lost in Transplantation: Characterizing Racial Gaps in Physician Organ Offer Acceptance
- PMID: 39072010
- PMCID: PMC11275659
- DOI: 10.1101/2024.07.14.24310395
Lost in Transplantation: Characterizing Racial Gaps in Physician Organ Offer Acceptance
Abstract
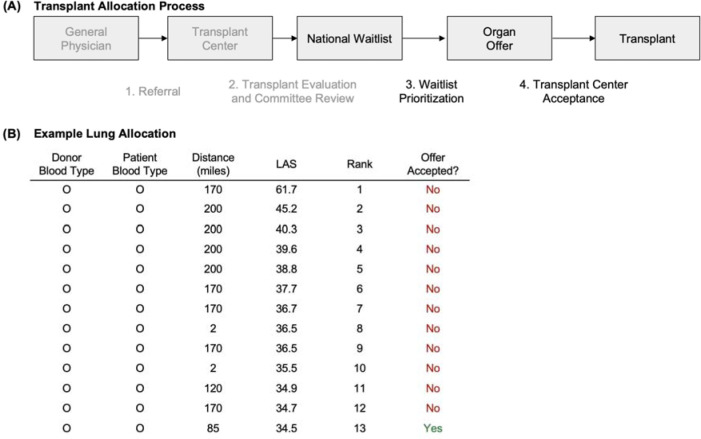
Background: There are known racial disparities in the organ transplant allocation system in the United States. However, prior work has yet to establish if transplant center decisions on offer acceptance-the final step in the allocation process-contribute to these disparities.
Objective: To estimate racial differences in the acceptance of organ offers by transplant center physicians on behalf of their patients.
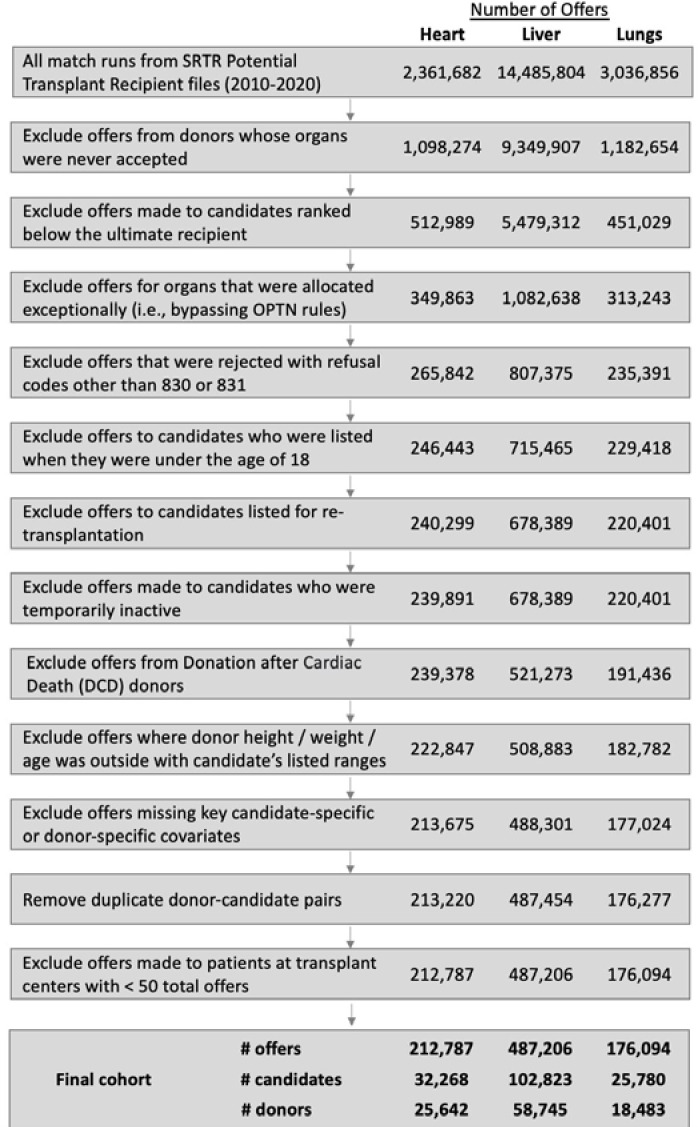
Design: Retrospective cohort analysis using data from the Scientific Registry of Transplant Recipients (SRTR) on patients who received an offer for a heart, liver, or lung transplant between January 1, 2010 and December 31, 2020.
Setting: Nationwide, waitlist-based.
Patients: 32,268 heart transplant candidates, 102,823 liver candidates, and 25,780 lung candidates, all aged 18 or older.
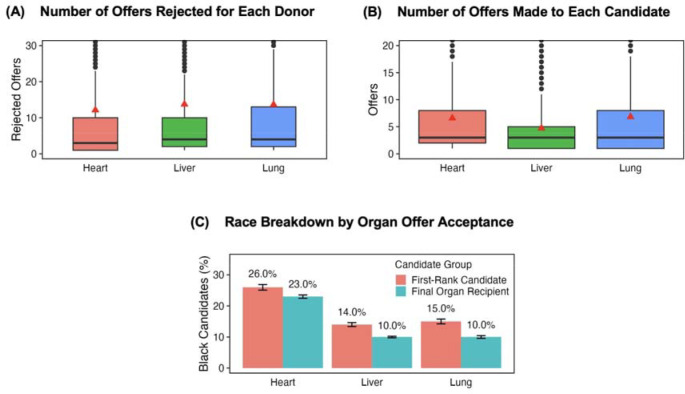
Measurements: 1) Association between offer acceptance and two race-based variables: candidate race and donor-candidate race match; 2) association between offer rejection and time to patient mortality.
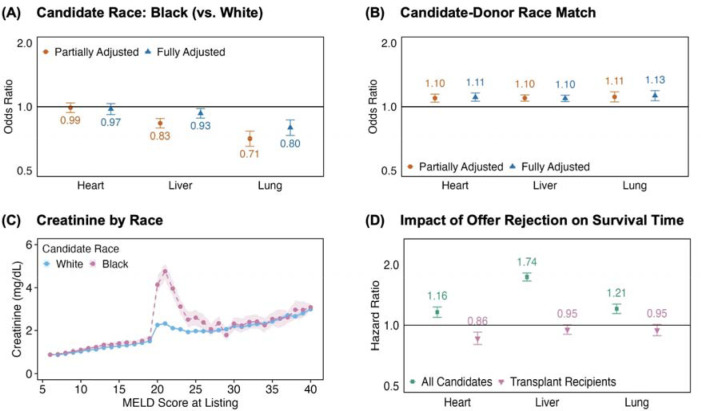
Results: Black race was associated with significantly lower odds of offer acceptance for livers (OR=0.93, CI: 0.88-0.98) and lungs (OR=0.80, CI: 0.73-0.87). Donor-candidate race match was associated with significantly higher odds of offer acceptance for hearts (OR=1.11, CI: 1.06-1.16), livers (OR=1.10, CI: 1.06-1.13), and lungs (OR=1.13, CI: 1.07-1.19). Rejecting an offer was associated with lower survival times for all three organs (heart hazard ratio=1.16, CI: 1.09-1.23; liver HR=1.74, CI: 1.66-1.82; lung HR=1.21, CI: 1.15-1.28).
Limitations: Our study analyzed the observational SRTR dataset, which has known limitations.
Conclusion: Offer acceptance decisions are associated with inequity in the organ allocation system. Our findings demonstrate the additional barriers that Black patients face in accessing organ transplants and demonstrate the need for standardized practice, continuous distribution policies, and better organ procurement.
Conflict of interest statement
Conflicts of interest Authors declare that they have no conflicts of interests.
Figures
References
-
- Based on OPTN data as of January 16, 2023.
-
- Nephew LD, Serper M. Racial, Gender, and Socioeconomic Disparities in Liver Transplantation. Liver Transpl. 2021;27(6):900–912. - PubMed
-
- Riley LE, Lascano J. Gender and racial disparities in lung transplantation in the United States. J Heart Lung Transplant. 2021;40(9):963–969. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources