

This is a preprint.
Identifying and Forecasting Importation and Asymptomatic Spreaders of Multi-drug Resistant Organisms in Hospital Settings
- PMID: 39072020
- PMCID: PMC11275683
- DOI: 10.1101/2024.07.14.24310393
Identifying and Forecasting Importation and Asymptomatic Spreaders of Multi-drug Resistant Organisms in Hospital Settings
Update in
-
Identifying and forecasting importation and asymptomatic spreaders of multi-drug resistant organisms in hospital settings.NPJ Digit Med. 2025 Mar 7;8(1):147. doi: 10.1038/s41746-025-01529-x. NPJ Digit Med. 2025. PMID: 40055525 Free PMC article.
Abstract
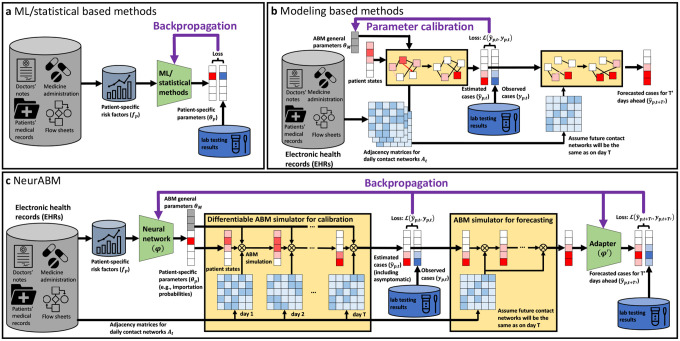
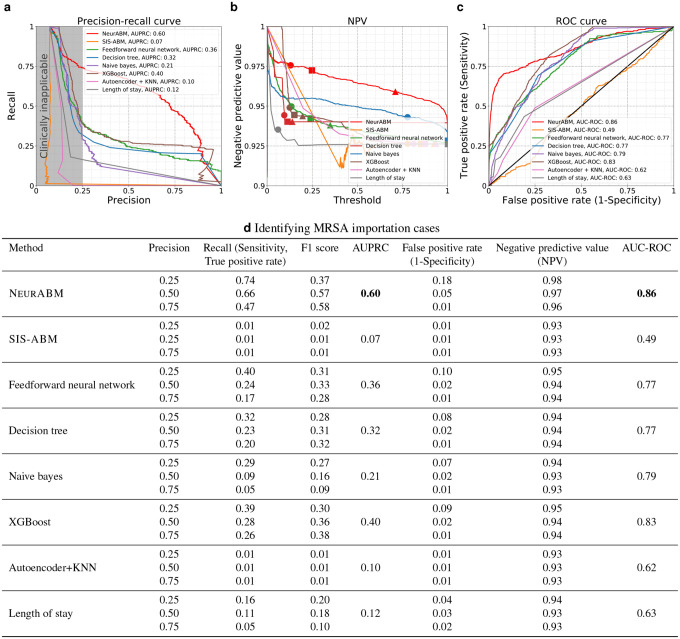
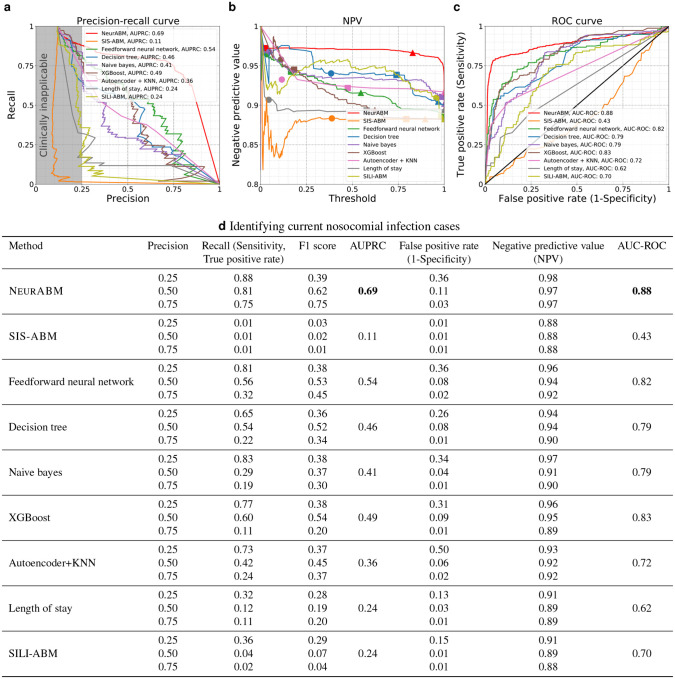
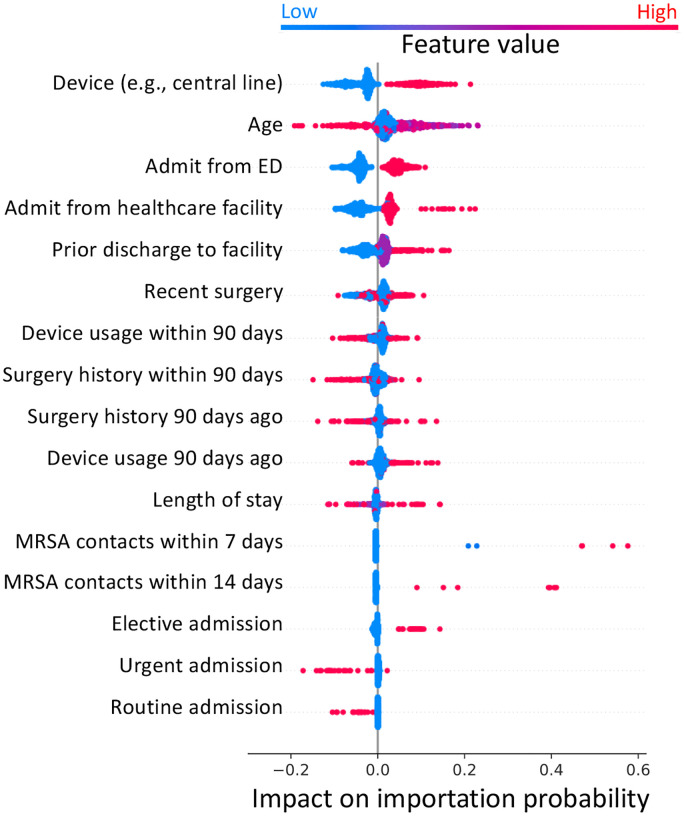
Healthcare-associated infections (HAIs) from multi-drug resistant organisms (MDROs) pose a significant challenge for healthcare systems. Patients can arrive at hospitals already infected ("importation") or acquire infections during their stay ("nosocomial infection"). Many cases, often asymptomatic, complicate rapid identification due to testing limitations and delays. Although recent advancements in mathematical modeling and machine learning have aimed to identify at-risk patients, these methods face challenges: transmission models often overlook valuable electronic health record (EHR) data, while machine learning approaches typically lack mechanistic insights into underlying processes. To address these issues, we propose NeurABM, a novel framework that integrates neural networks and agent-based models (ABM) to leverage the strengths of both methods. NeurABM simultaneously learns a neural network for patient-level importation predictions and an ABM for infection identification. Our findings show that NeurABM significantly outperforms existing methods, marking a breakthrough in accurately identifying importation cases and forecasting future nosocomial infections in clinical practice.
Conflict of interest statement
Competing Interests The authors declare no competing interests.
Figures


References
-
- Albrich W. C., and Harbarth S. Health-care workers: source, vector, or victim of mrsa? The Lancet infectious diseases 8, 5 (2008), 289–301. - PubMed
-
- Bhalla A., Pultz N. J., Gries D. M., Ray A. J., Eckstein E. C., Aron D. C., and Donskey C. J. Acquisition of nosocomial pathogens on hands after contact with environmental surfaces near hospitalized patients. Infection Control & Hospital Epidemiology 25, 2 (2004), 164–167. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources