

Approaches to Treating High Risk and Advanced Renal Cell Carcinoma (RCC): Key Trial Data That Impacts Treatment Decisions in the Clinic
- PMID: 39072353
- PMCID: PMC11282163
- DOI: 10.2147/RRU.S457287
Approaches to Treating High Risk and Advanced Renal Cell Carcinoma (RCC): Key Trial Data That Impacts Treatment Decisions in the Clinic
Abstract
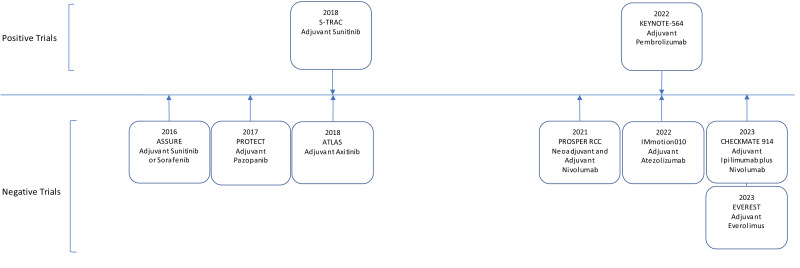
The treatment paradigm for high risk localized and advanced kidney cancer has been characterized by ongoing changes, with the introduction of vascular endothelial growth factor receptor tyrosine kinase inhibitors (VEGFR TKIs) and later with immune checkpoint blockade. In this article, we review how current evidence informs our decision-making on post-checkpoint inhibitor systemic therapies, the role of adjuvant and/or neoadjuvant therapies, and the role of cytoreductive nephrectomy in the evolving systemic therapy landscape. While some studies support a post-checkpoint inhibitor benefit from the VEGFR TKIs cabozantinib or axitinib, the benefit of doublet therapies including a VEGF receptor inhibitor and a checkpoint inhibitor remains an area of active investigation, with the combination of lenvatinib plus pembrolizumab showing promise but with a Phase III trial of the combination of atezolizumab plus cabozantinib showing no benefit over cabozantinib alone. The role of adjuvant therapy in patients with high-risk disease who have undergone cytoreductive nephrectomy and potentially metastasectomy is also an area of continuing interest. While the S-TRAC study demonstrated a disease-free survival benefit for adjuvant sunitinib, no overall survival benefit was shown, and multiple other studies of adjuvant VEGFR TKI therapy have been negative. Subsequently, adjuvant pembrolizumab has shown a benefit in overall survival, whereas trials of neoadjuvant and adjuvant nivolumab, adjuvant atezolizumab, and adjuvant ipilimumab plus nivolumab have all been negative. Finally, the role for cytoreductive nephrectomy continues to be an area of active debate. The CARMENA study raised important questions about the role of cytoreductive nephrectomy given the advances in VEGFR TKI therapy but was characterized by accrual difficulties and a significant number of patients not receiving treatment according to the study protocol. Two ongoing studies (NORDIC-SUN and PROBE) seek to further address the role of cytoreductive nephrectomy in the doublet therapy era.
Keywords: adjuvant therapy; cytoreductive nephrectomy; immunotherapy; kidney cancer.
© 2024 Chatzkel et al.
Conflict of interest statement
Dr Jonathan Chatzkel supported investigator initiated clinical trial at the University of Florida for Genentech and Aveo Oncology, outside the submitted work. Dr Mayer Fishman reports personal fees for DSMB from Immatics and Carsgen; personal fees for consulting from Bayer and Pfizer; personal fees for education program from DAVA, outside the submitted work. Dr Padraic O’Malley reports personal fees for consulting from Intuitive Surgical, outside the submitted work. Dr Guru Sonpavde reports grants and/or personal fees for advisory board/consultant and/or speaker from BMS, Exelixis, Merck, Pfizer, Bayer, during the conduct of the study; grants and/or personal fees from EMD Serono, Seagen, Janssen, Bicycle Therapeutics, Gilead, Scholar Rock, G1 Therapeutics, Servier, Syncorp, Jazz Therapeutics, Natera, Aveo, outside the submitted work. The authors report no other conflicts of interest in this work.
Figures
References
LinkOut - more resources
Full Text Sources
