

Prenatal parvovirus B19 infection
- PMID: 39073431
- PMCID: PMC11485125
- DOI: 10.1007/s00404-024-07644-6
Prenatal parvovirus B19 infection
Abstract
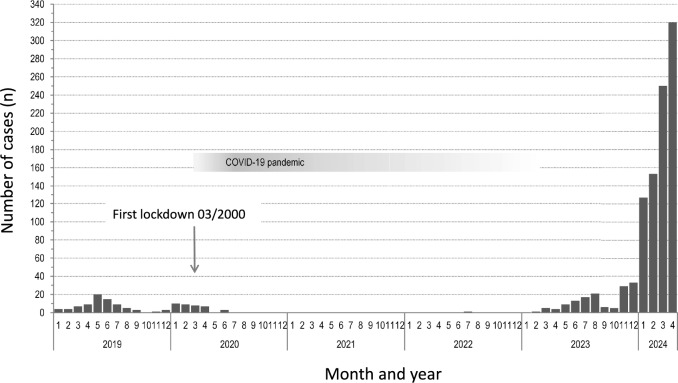
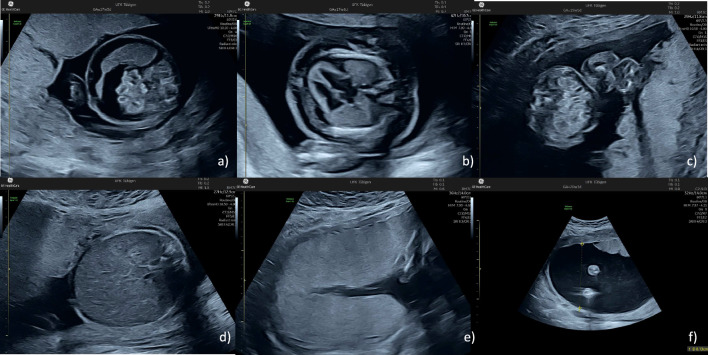
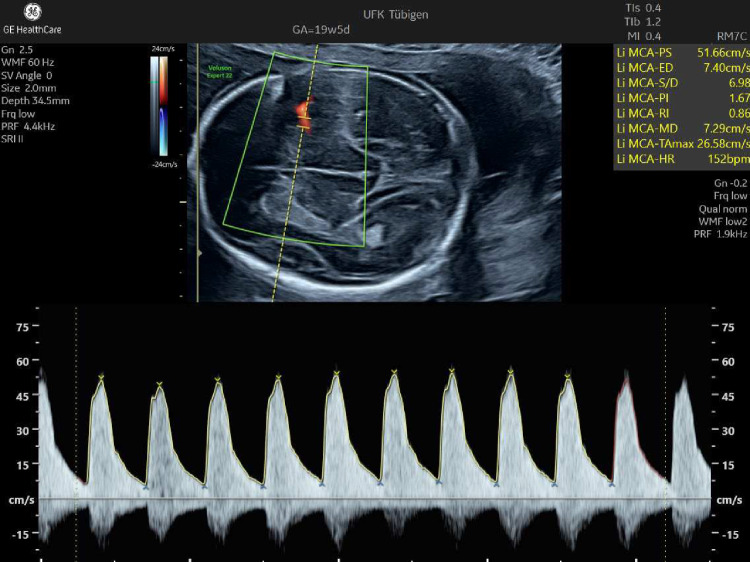
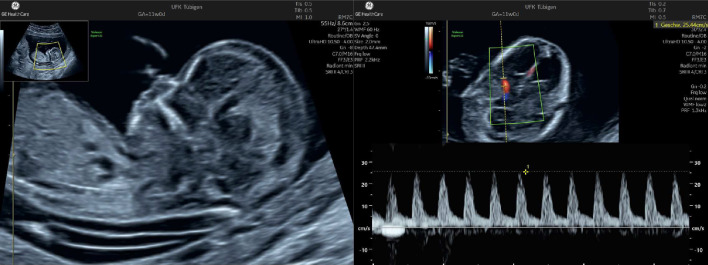
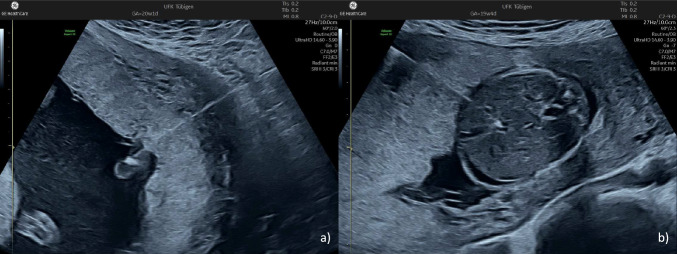
Parvovirus B19 (B19V) causes erythema infectiosum, a.k.a., fifth disease. This disease primarily affects children. It is generally self-limiting and subsides after 1-2 weeks. In pregnancy, the virus can cross the placenta and result in a fetal infection. This may lead to severe fetal anemia, hydrops fetalis, a miscarriage, or intrauterine fetal death. The risk of long-term sequelae also appears to be increased. About one-third of pregnant women are not immune to B19V and, therefore, are at risk to contract a primary infection. The seroconversion rate during pregnancy is generally around 1-2%. During a primary infection, maternal-fetal transplacental transmission of B19V occurs in about 30-50% of the cases and the risk of fetal infection increases with advancing gestational age. The risk of severe fetal anemia or hydrops is around 3-4% overall and is around 6-7% if the primary infection occurs before 20 weeks' gestation. Fetal monitoring in women with a primary B19V infection includes regular ultrasound examinations looking for evidence of hydrops fetalis and Doppler measurements of the middle cerebral artery peak velocity. Fetal blood sampling is performed if a significant anemia is suspected and, if such is found, an intrauterine blood transfusion is needed. This article provides an overview of the epidemiology, pathogenesis, clinical manifestations, diagnostic methods, and management of B19V infection during pregnancy.
Keywords: Anemia; Hydrops; Infection; Parvovirus B19; Prenatal.
© 2024. The Author(s).
Conflict of interest statement
Karl Oliver Kagan, Annegret Geipel and Jiri Sonek are editors of the Archives of Gynecology and Obstetrics. Karl Oliver Kagan is the Editor in Chief.
Figures


References
-
- Beck R, Exler S, Enders M (2024) Parvovirus B19-Infektion und Schwangerschaft. Epid Bull 24:3–7. 10.25646/12157
-
- S2k-Leitlinie - Labordiagnostik schwangerschaftsrelevanter Virusinfektionen. AWMF Registernummer 093/001. https://register.awmf.org/de/leitlinien/detail/093-001. Accessed 1 July 2024
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
