

Goal-directed osteoporosis treatment: ASBMR/BHOF task force position statement 2024
- PMID: 39073912
- PMCID: PMC11425703
- DOI: 10.1093/jbmr/zjae119
Goal-directed osteoporosis treatment: ASBMR/BHOF task force position statement 2024
Abstract
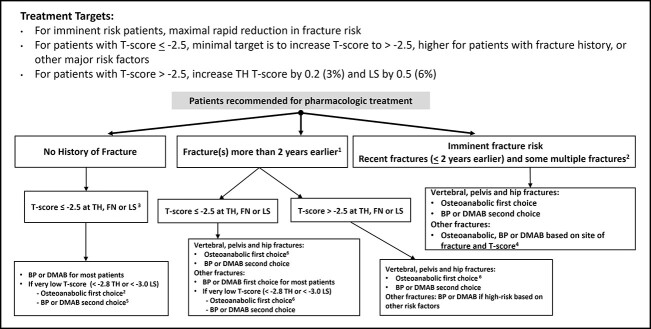
The overarching goal of osteoporosis management is to prevent fractures. A goal-directed approach to long-term management of fracture risk helps ensure that the most appropriate initial treatment and treatment sequence is selected for individual patients. Goal-directed treatment decisions require assessment of clinical fracture history, vertebral fracture identification (using vertebral imaging as appropriate), measurement of bone mineral density (BMD), and consideration of other major clinical risk factors. Treatment targets should be tailored to each patient's individual risk profile and based on the specific indication for beginning treatment, including recency, site, number and severity of prior fractures, and BMD levels at the total hip, femoral neck, and lumbar spine. Instead of first-line bisphosphonate treatment for all patients, selection of initial treatment should focus on reducing fracture risk rapidly for patients at very high and imminent risk, such as in those with recent fractures. Initial treatment selection should also consider the probability that a BMD treatment target can be attained within a reasonable period of time and the differential magnitude of fracture risk reduction and BMD impact with osteoanabolic versus antiresorptive therapy. This position statement of the ASBMR/BHOF Task Force on Goal-Directed Osteoporosis Treatment provides an overall summary of the major clinical recommendations about treatment targets and strategies to achieve those targets based on the best evidence available, derived primarily from studies in older postmenopausal women of European ancestry.
Keywords: DXA, analysis/quantitation of bone; anabolics, therapeutics; antiresorptives, therapeutics; osteoporosis, diseases and disorders of/related to bone; practice/policy-related issues.
Plain language summary
Goal-directed treatment can help healthcare providers recommend the best treatments for individual patients to prevent fractures. The goal-directed strategy considers the site, number, and recency of prior fractures. This may require imaging for spine fractures, which may not have caused pain. Treatment decisions also require bone mineral density (BMD) measurement and consideration of other major risk factors. In contrast to the standard approach, same first treatment for all, treatment selection is tailored to an individual’s risk. In patients with recent fractures of the spine, hip, or pelvis, fracture risk is very high and treatment should rapidly reduce that risk. For others, the target is a specific BMD level and should consider the likelihood that the treatment target can be attained within a reasonable period of time, which differs for osteoporosis medications. After initial therapy, BMD should be assessed to determine if the target has been achieved. If so, strategies should focus on maintaining BMD. If the target is not yet achieved, treatment should be intensified, or continued if it is already the most potent option. This position statement represents a consensus of expert recommendations about treatment targets and strategies to achieve those targets based on the best available evidence.
© The Author(s) 2024. Published by Oxford University Press on behalf of the American Society for Bone and Mineral Research.
Conflict of interest statement
F.C.: Amgen: investigator, consultant, advisor, speaker; Radius Health: investigator, consultant, speaker; Enterabio, Biocon, CuraTeQ, Pfizer/Myovant/Sumitomo, Theramex, UCB: consultant.
E.M.L.: Amgen: investigator, consultant, speaker; Radius: investigator, consultant; Ultragenyx: investigator; Kyowa Kirin: consultant, speaker; Angitia and Ascendis: consultant.
R.E.
P.R.E.
S.J.d.B.
B.L.
Y.R.
D.P.K.: Amgen: grant funds, Radius Health: consultant and grant funds, Agnovos: Data and Safety Monitoring Board.
G.E.H.F.: None.
J.T.S.
J.L.C.B.
A.C.
A.D.P.: Theramex: speaker and advisor.
P.H.: Amgen, Besins, Exeltis, Gedeon Richter, Hexal, Sandoz, Stada, Theramex and UCB: speaker and consultant.
S.T.
F.T.
W.X.
S.R.C.
Figures
References
-
- Camacho PM, Petak SM, Binkley N, et al. American Association of Clinical Endocrinologists/American College of Endocrinology clinical practice guidelines for the diagnosis and treatment of postmenopausal osteoporosis—2020 update. Endocr Pract. 2020;26(Suppl 1):1–46. 10.4158/GL-2020-0524SUPPL - DOI - PubMed
-
- Kanis JA, Cooper C, Rizzoli R, Reginster JY, Scientific Advisory Board of the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO) and the Committees of Scientific Advisors and National Societies of the International Osteoporosis Foundation (IOF) . Executive summary of European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Aging Clin Exp Res. 2019;31(1):15–17. 10.1007/s40520-018-1109-4 - DOI - PubMed
-
- Management of Osteoporosis in Postmenopausal Women: The 2021 Position Statement of the North American Menopause Society Editorial Panel . Management of osteoporosis in postmenopausal women: the 2021 position statement of the North American Menopause Society. Menopause. 2021;28(9):973–997. 10.1097/GME.0000000000001831 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
