

Japanese classification of pancreatic carcinoma by the Japan Pancreas Society: Eighth edition
- PMID: 39074998
- PMCID: PMC11589393
- DOI: 10.1002/jhbp.12056
Japanese classification of pancreatic carcinoma by the Japan Pancreas Society: Eighth edition
Abstract
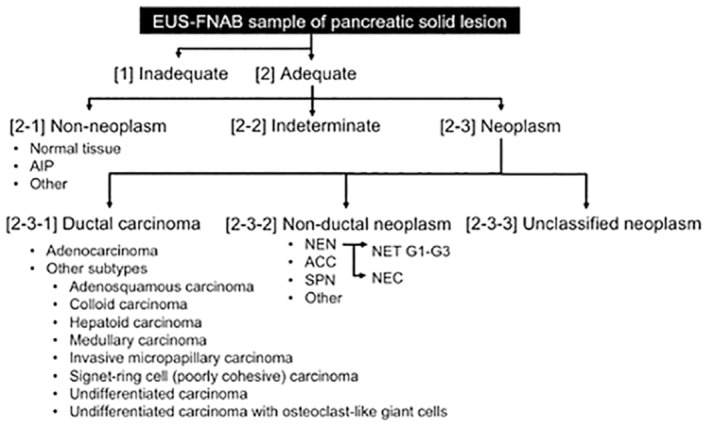
In 2023, the Japan Pancreas Society (JPS) published the new eighth edition of the Japanese classification of pancreatic carcinoma. We present here an excerpted version in English, based on the latest edition. The major changes in this revision are as follows: In the eighth edition of the Union for International Cancer Control (UICC), the T category was changed to be based on tumor size; however, the eighth edition of the Japanese classification retains the previous T category based on local invasion factors. Lymph nodes have been renamed, and regional lymph nodes have been defined by location. Peritoneal cytology, which was not previously included in distant metastasis (M), has now been included in the M category. Moreover, significant additions have been made regarding the pathological diagnosis of endoscopic ultrasound-guided fine-needle aspiration biopsy (EUS-FNAB) and criteria for histological assessment of the effects after chemotherapy and radiation therapy. Although this classification is aimed at carcinoma originating in the pancreas, not in the bile duct or duodenum, if the differentiation of the primary organ is difficult, this classification should be applied. It is also desirable to describe tumors other than carcinoma and metastatic tumors to the pancreas in accordance with this classification.
Keywords: Japanese; classification; neoplasm staging; pancreatic cancer; pancreatic neoplasms.
© 2024 The Author(s). Journal of Hepato‐Biliary‐Pancreatic Sciences published by John Wiley & Sons Australia, Ltd on behalf of Japanese Society of Hepato‐Biliary‐Pancreatic Surgery.
Conflict of interest statement
The authors declare there are no conflicts of interest.
Figures
References
-
- Japan Pancreas Society . Japanese classification of pancreatic carcinoma. 1st ed. Tokyo: Kanehara; 1980. (in Japanese).
-
- Japan Pancreas Society . Japanese classification of pancreatic carcinoma. 8th ed. Tokyo: Kanehara; 2023. (in Japanese).
-
- Japan Pancreas Society . Japanese classification of pancreatic carcinoma. 7th ed. Tokyo: Kanehara; 2016. (in Japanese).
-
- Tsuchida H, Fujii T, Mizuma M, Satoi S, Igarashi H, Eguchi H, et al. Prognostic importance of peritoneal washing cytology in patients with otherwise resectable pancreatic ductal adenocarcinoma who underwent pancreatectomy: a nationwide, cancer registry‐based study from the Japan pancreas society. Surgery. 2019;166:997–1003. - PubMed
-
- Yoshioka H, Wakabayashi T. Procedure of neurotomy on the head of the pancreas (in Japanese). Shujutsu Oper. 1957;11:849–857.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
