

Modifiable lifestyle factors and the risk of post-COVID-19 multisystem sequelae, hospitalization, and death
- PMID: 39075060
- PMCID: PMC11286928
- DOI: 10.1038/s41467-024-50495-7
Modifiable lifestyle factors and the risk of post-COVID-19 multisystem sequelae, hospitalization, and death
Abstract
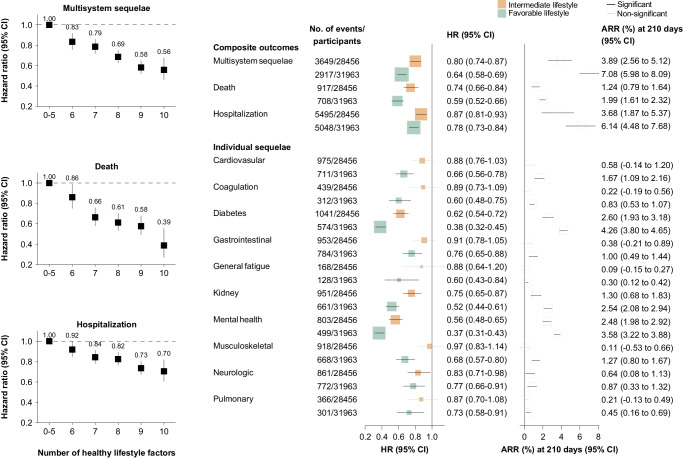
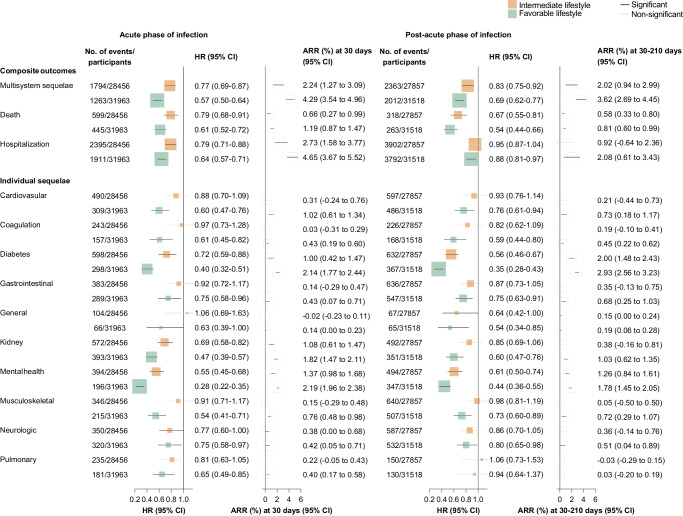
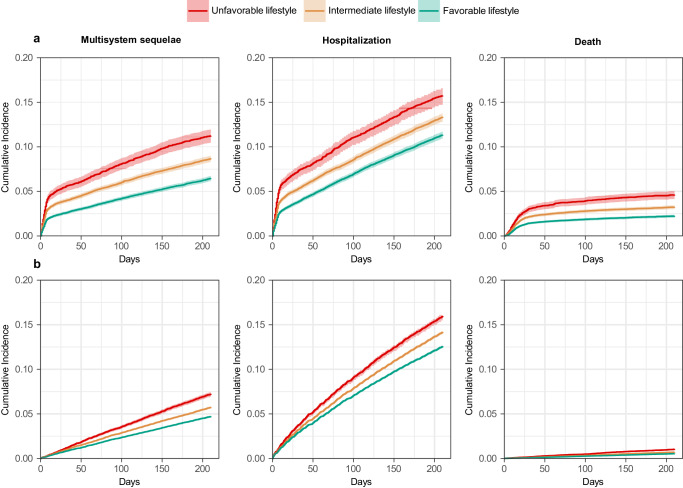
Effective prevention strategies for post-COVID complications are crucial for patients, clinicians, and policy makers to mitigate their cumulative burden. This study evaluated the association of modifiable lifestyle factors (smoking, alcohol intake, BMI, physical activity, sedentary time, sleep duration, and dietary habits) with COVID-19 multisystem sequelae, death, and hospitalization in the UK Biobank cohort (n = 68,896). A favorable lifestyle (6-10 healthy factors; 46.4%) was associated with a 36% lower risk of multisystem sequelae (HR, 0.64; 95% CI, 0.58-0.69; ARR at 210 days, 7.08%; 95% CI, 5.98-8.09) compared to an unfavorable lifestyle (0-4 factors; 12.3%). Risk reductions spanned all 10 organ systems, including cardiovascular, coagulation, metabolic, gastrointestinal, kidney, mental health, musculoskeletal, respiratory disorders, and fatigue. This beneficial effect was largely attributable to direct lifestyle impacts independent of corresponding pre-infection comorbidities (71% for any sequelae). A favorable lifestyle was also related to the risk of post-COVID death (HR 0.59, 0.52-0.66) and hospitalization (HR 0.78, 0.73-0.84). These associations persisted across acute and post-acute infection phases, irrespective of hospitalization status, vaccination, or SARS-CoV-2 variant. These findings underscore the clinical and public health importance of adhering to a healthy lifestyle in mitigating long-term COVID-19 adverse impacts and enhancing future pandemic preparedness.
© 2024. The Author(s).
Conflict of interest statement
D.P.-A. reported grants from Amgen, UCB Biopharma, Les Laboratoires Servier, Novartis, and Chiesi-Taylor, as well as speaker fees and advisory board membership with AstraZeneca and Johnson and Johnson outside the submitted work, in addition to research support from Janssen. R.P. has participated in advisory boards for Gilead, MSD, ViiV Healthcare, Theratechnologies and Lilly. His institution has received research support from Gilead, MSD, and ViiV Healthcare. The remaining authors declare no competing interests.
Figures


References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
