

Peripheral inflammation is associated with brain atrophy and cognitive decline linked to mild cognitive impairment and Alzheimer's disease
- PMID: 39075118
- PMCID: PMC11286782
- DOI: 10.1038/s41598-024-67177-5
Peripheral inflammation is associated with brain atrophy and cognitive decline linked to mild cognitive impairment and Alzheimer's disease
Abstract
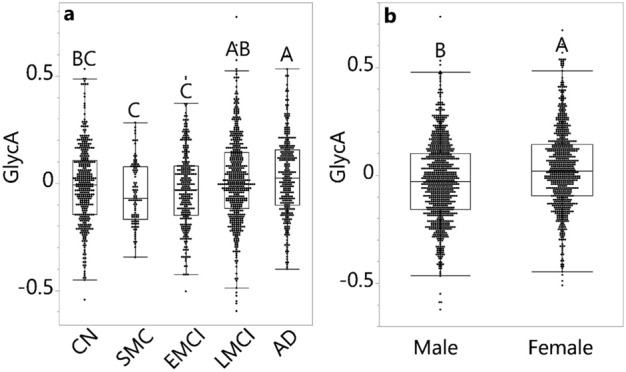
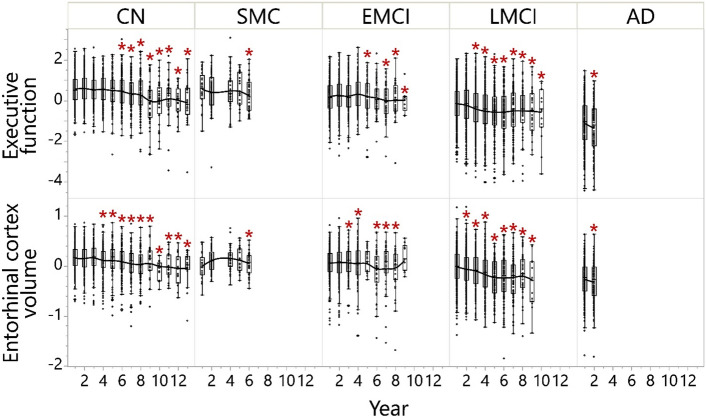
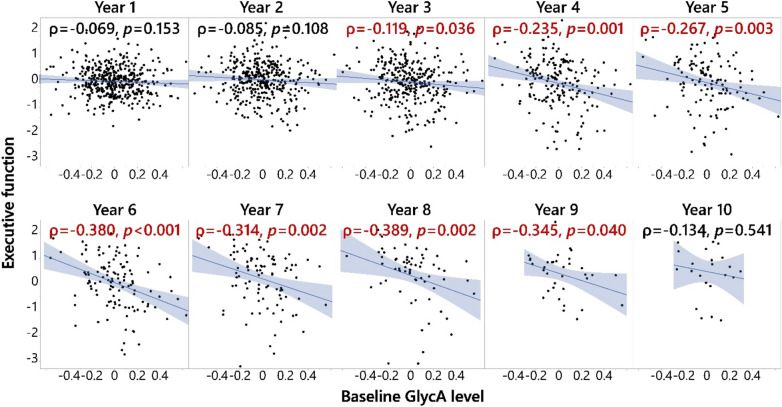
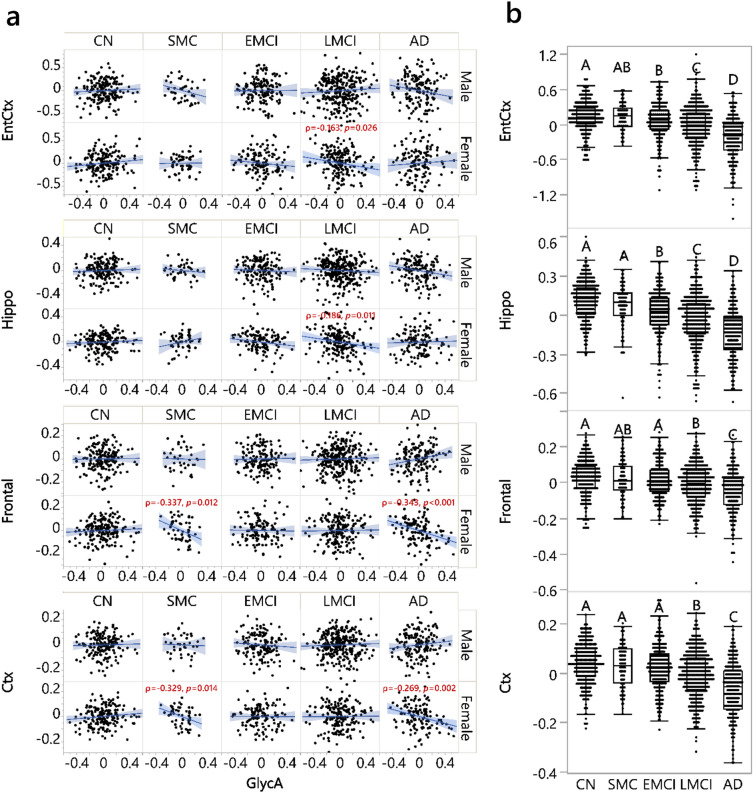
Inflammation is an important factor in Alzheimer's disease (AD). An NMR measurement in plasma, glycoprotein acetyls (GlycA), captures the overall level of protein production and glycosylation implicated in systemic inflammation. With its additional advantage of reducing biological variability, GlycA might be useful in monitoring the relationship between peripheral inflammation and brain changes relevant to AD. However, the associations between GlycA and these brain changes have not been fully evaluated. Here, we performed Spearman's correlation analyses to evaluate these associations cross-sectionally and determined whether GlycA can inform AD-relevant longitudinal measurements among participants in the Alzheimer's Disease Neuroimaging Initiative (n = 1506), with additional linear models and stratification analyses to evaluate the influences of sex or diagnosis status and confirm findings from Spearman's correlation analyses. We found that GlycA was elevated in AD patients compared to cognitively normal participants. GlycA correlated negatively with multiple concurrent regional brain volumes in females diagnosed with late mild cognitive impairment (LMCI) or AD. Baseline GlycA level was associated with executive function decline at 3-9 year follow-up in participants diagnosed with LMCI at baseline, with similar but not identical trends observed in the future decline of memory and entorhinal cortex volume. Results here indicated that GlycA is an inflammatory biomarker relevant to AD pathogenesis and that the stage of LMCI might be relevant to inflammation-related intervention.
Keywords: Alzheimer’s disease; Brain atrophy; GlycA; Inflammation; Inflammatory biomarker; Metabolomics; Mild cognitive impairment; Peripheral-central connection; Population heterogeneity; Sex differences.
© 2024. The Author(s).
Conflict of interest statement
Dr. Rima Kaddurah-Daouk and Dr. Matthias Arnold participated in the invention of several patents on applying metabolomics to diagnose and treat CNS diseases. Dr. Kaddurah-Daouk holds equity in Metabolon Inc., Chymia LLC and PsyProtix, which were not involved in the current study. Dr. Arnold holds equity in Chymia LLC and IP in PsyProtix. All other authors declare that they have no competing interests.
Figures

References
MeSH terms
Substances
Grants and funding
- R01 AG046171/AG/NIA NIH HHS/United States
- U01 AG072177/AG/NIA NIH HHS/United States
- U19 AG074879/AG/NIA NIH HHS/United States
- RF1AG057452/AG/NIA NIH HHS/United States
- P30AG072972/NH/NIH HHS/United States
- 3U19AG063744-04S1/AG/NIA NIH HHS/United States
- U19AG063744/AG/NIA NIH HHS/United States
- U01AG061359/AG/NIA NIH HHS/United States
- NIA R01AG046171/AG/NIA NIH HHS/United States
- RF1 AG057452/AG/NIA NIH HHS/United States
- R01 AG081322/AG/NIA NIH HHS/United States
- P30 AG072972/AG/NIA NIH HHS/United States
- U01 AG072177/NH/NIH HHS/United States
- RF1AG058942/AG/NIA NIH HHS/United States
- Project 2032-51530-025-00D/United States Department of Agriculture
- R01AG059093/AG/NIA NIH HHS/United States
- RF1AG051550/AG/NIA NIH HHS/United States
- U19AG074879/NH/NIH HHS/United States
- FNIH: #DAOU16AMPA/AG/NIA NIH HHS/United States
- U19 AG063744/AG/NIA NIH HHS/United States
- 1R01AG081322/AG/NIA NIH HHS/United States
- 2009965/National Health and Medical Research Council of Australia
- R01 AG015903/AG/NIA NIH HHS/United States
- RF1 AG059093/AG/NIA NIH HHS/United States
- R01 LM012535/NH/NIH HHS/United States
- R01 LM012535/LM/NLM NIH HHS/United States
- U01 AG061359/AG/NIA NIH HHS/United States
- RF1 AG058942/AG/NIA NIH HHS/United States
- RF1 AG051550/AG/NIA NIH HHS/United States
