

Impact of Nodular Calcifications in the Aortic Annulus and Left Ventricular Outflow Tract on TAVI Outcome with New-Generation Devices
- PMID: 39076178
- PMCID: PMC11269076
- DOI: 10.31083/j.rcm2311358
Impact of Nodular Calcifications in the Aortic Annulus and Left Ventricular Outflow Tract on TAVI Outcome with New-Generation Devices
Abstract
Background: The impact of nodular calcifications in left ventricular outlow tract (LVOT) and aortic annulus on the procedural outcome of transcatheter aortic valve implantation (TAVI) with new-generation devices is yet to be elucidated. Similarly, computational simulations may provide a novel insight into the biomechanical features of TAVI devices and their interaction with nodular calcifications.
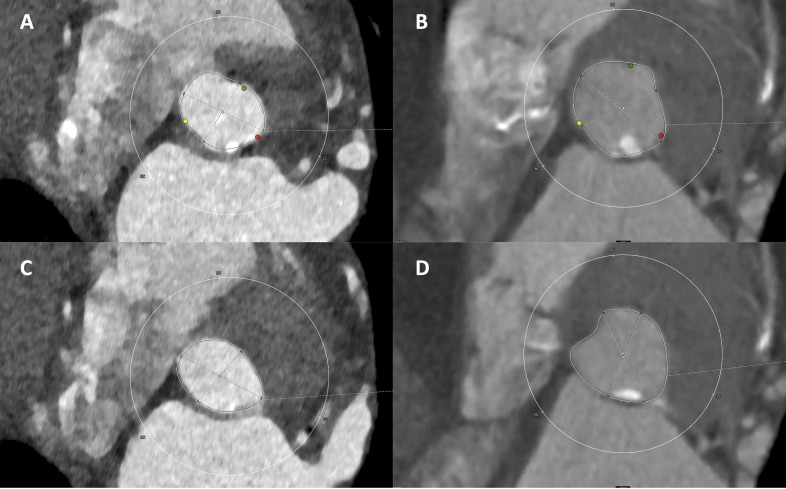
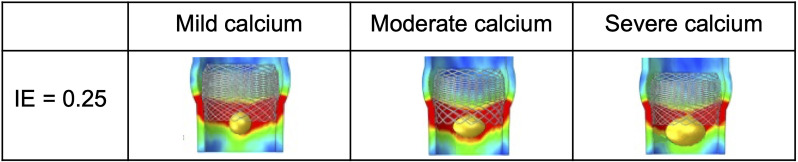
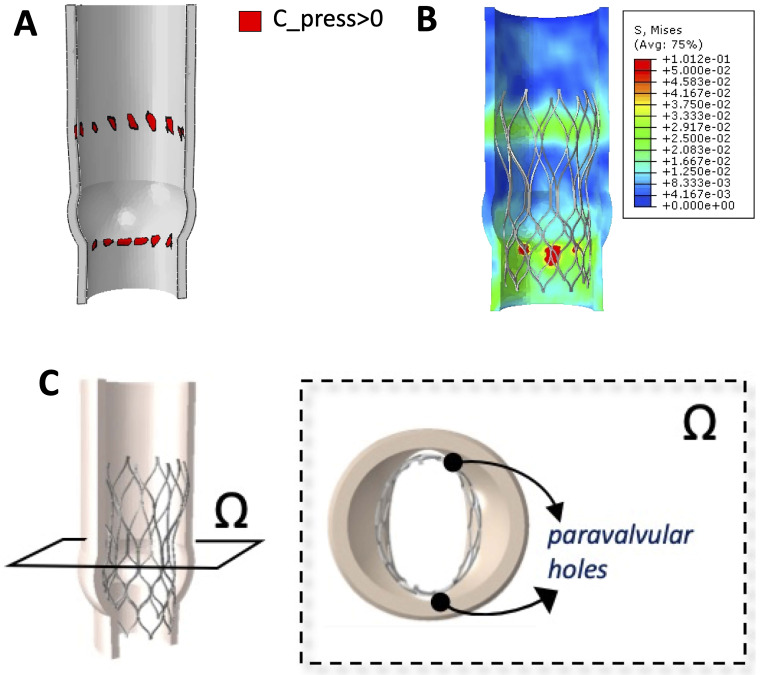
Methods: This retrospective single-center study included 232 patients submitted to TAVI with Evolut-R (53.4%), Portico (33.6%) and Lotus (13.0%) devices with available preoperative computed tomography (CT) angiography and evidence of nodular calcifications in aortic annulus and/or LVOT. Calcification severity was defined moderate in presence of at least two nodules or one nodule 5 mm. Three virtual simulation models of aortic root presenting a nodular calcification of increasing size were implemented. Stress distribution, stent-root contact area and paravalvular orifice area were computed.
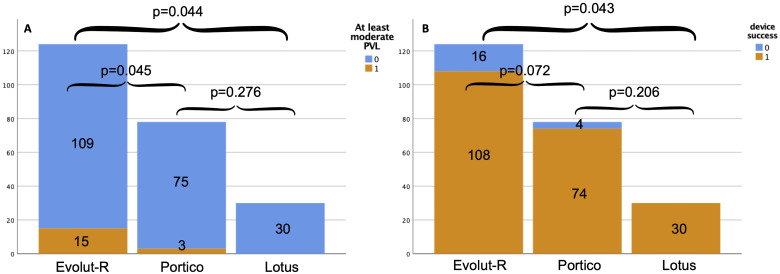
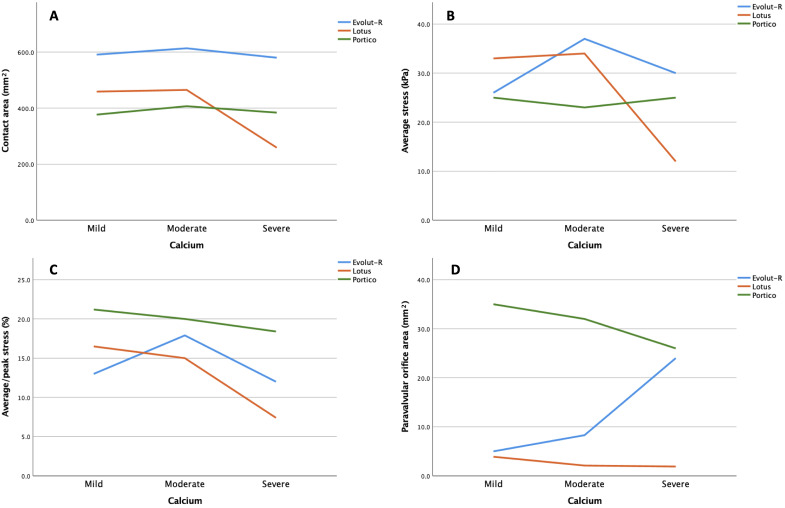
Results: At least moderate calcifications were found in 123 (53.0%) patients, with no sex differences. Among the moderate calcification group, lower device success rate was evident (87.8% vs. 95.4%; p = 0.039). Higher rates of moderate paravalvular leak (PVL) (11.4% vs. 3.7%; p = 0.028) and vascular complications (9.8% vs. 2.8%; p = 0.030) were also observed. Among the Evolut-R group, higher rates of at moderate PVL (12.1%) were observed compared to Portico (3.8%; p = 0.045) and Lotus (0.0%; p = 0.044) groups. Calcification of both annulus and LVOT (odds ratio [OR] 0.105; p = 0.023) were independent predictors of device success. On computational simulations, Portico exhibited homogeneous stress distribution by increasing calfications and overall a larger paravalvular orifice areas compared to Evolut-R and Lotus. Evolut-R showed higher values of average stress than Portico, although with a more dishomogeneous distribution leading to greater paravalvular orifice areas by severe calcifications. Lotus showed overall small paravalvular orifice areas, with no significant increase across the three models.
Conclusions: At least moderate nodular calcifications in the annulus/LVOT region significantly affected TAVI outcome, as they were independent predictors of device success. Lotus and Portico seemed to perform better than Evolut-R as for device success and moderate PVL. Computational simulations revealed unique biomechanical features of the investigated devices in terms of stent compliance and radial force.
Keywords: computational simulation; device success; nodular calcification; paravalvular leak; transcatheter aortic valve implantation.
Copyright: © 2022 The Author(s). Published by IMR Press.
Conflict of interest statement
Francesco Bedogni is consultant for Medtronic, Abbott, and Boston Scientific; Nedy Brambilla and Luca Testa are consultants for Abbott and Boston Scientific. The other authors declare no conflict of interest.
Figures
Similar articles
-
Impact of aortic angle on transcatheter aortic valve implantation outcome with Evolut-R, Portico, and Acurate-NEO.Catheter Cardiovasc Interv. 2021 Jan 1;97(1):E135-E145. doi: 10.1002/ccd.28957. Epub 2020 May 13. Catheter Cardiovasc Interv. 2021. PMID: 32400068
-
Outcome of transcatheter aortic valve replacement in bicuspid aortic valve stenosis with new-generation devices.Interact Cardiovasc Thorac Surg. 2021 Jan 1;32(1):20-28. doi: 10.1093/icvts/ivaa231. Interact Cardiovasc Thorac Surg. 2021. PMID: 33201993 Free PMC article.
-
Early Clinical Outcomes of Transcatheter Aortic Valve Replacement in Left Ventricular Outflow Tract Calcification: New-Generation Device vs Early-Generation Device.J Invasive Cardiol. 2018 Nov;30(11):421-427. J Invasive Cardiol. 2018. PMID: 30373952
-
Impact of left ventricle outflow tract calcification on the outcomes of transcatheter aortic valve implantation: A study-level meta-analysis.J Card Surg. 2022 May;37(5):1379-1390. doi: 10.1111/jocs.16306. Epub 2022 Feb 13. J Card Surg. 2022. PMID: 35152472 Review.
-
How valvular calcification can affect the outcomes of transcatheter aortic valve implantation.Expert Rev Med Devices. 2020 Aug;17(8):773-784. doi: 10.1080/17434440.2020.1789456. Epub 2020 Jul 13. Expert Rev Med Devices. 2020. PMID: 32597265 Review.
Cited by
-
Impact of burden and distribution of aortic valve calcification on the hemodynamic performance and procedural outcomes of a self-expanding, intra-annular transcatheter aortic valve system.Int J Cardiovasc Imaging. 2024 Dec;40(12):2545-2558. doi: 10.1007/s10554-024-03261-1. Epub 2024 Oct 21. Int J Cardiovasc Imaging. 2024. PMID: 39432134
References
-
- Mack MJ, Leon MB, Smith CR, Miller DC, Moses JW, Tuzcu EM, et al. 5-year outcomes of transcatheter aortic valve replacement or surgical aortic valve replacement for high surgical risk patients with aortic stenosis (PARTNER 1): a randomised controlled trial. The Lancet . 2015;385:2477–2484. - PubMed
-
- Leon MB, Smith CR, Mack MJ, Makkar RR, Svensson LG, Kodali SK, et al. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. The New England Journal of Medicine . 2016;374:1609–1620. - PubMed
-
- Popma JJ, Deeb GM, Yakubov SJ, Mumtaz M, Gada H, O’Hair D, et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. The New England Journal of Medicine . 2019;380:1706–1715. - PubMed
-
- Mack MJ, Leon MB, Thourani VH, Makkar R, Kodali SK, Russo M, et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. The New England Journal of Medicine . 2019;380:1695–1705. - PubMed
-
- Choudhury T, Solomonica A, Bagur R. The Evolut R and Evolut PRO transcatheter aortic valve systems. Expert Review of Medical Devices . 2019;16:3–9. - PubMed
LinkOut - more resources
Full Text Sources
