

Cardiorespiratory Fitness in the Prevention and Management of Cardiovascular Disease
- PMID: 39076181
- PMCID: PMC11269081
- DOI: 10.31083/j.rcm2311382
Cardiorespiratory Fitness in the Prevention and Management of Cardiovascular Disease
Abstract
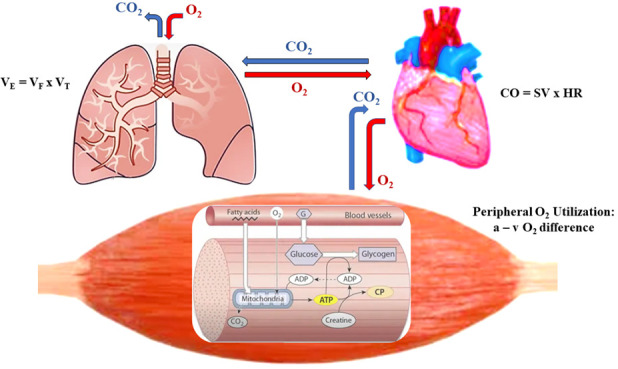
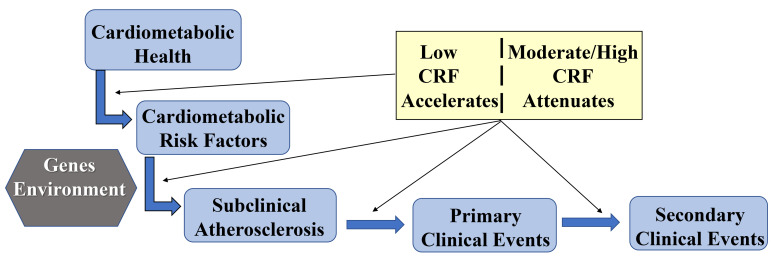
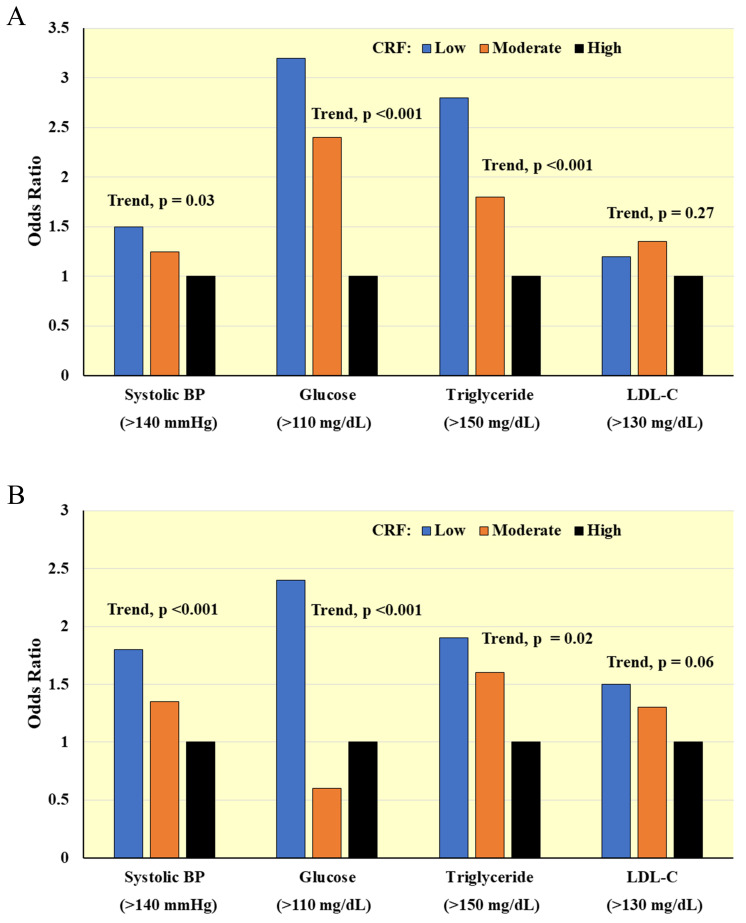
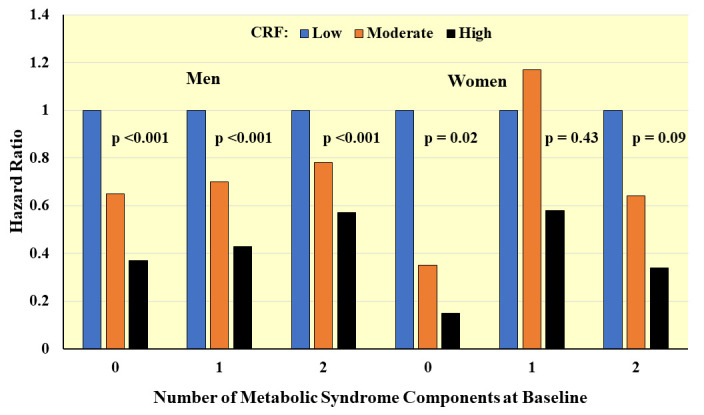
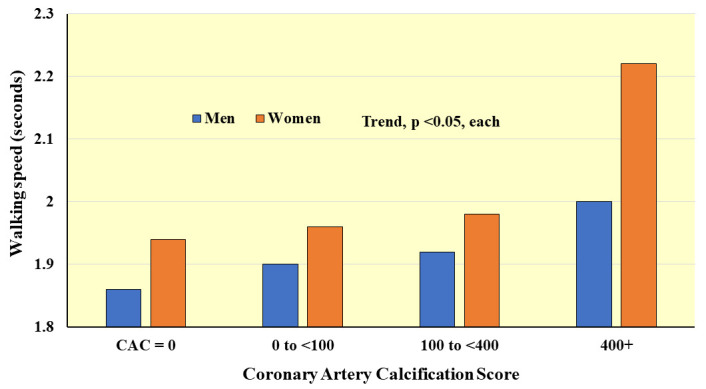
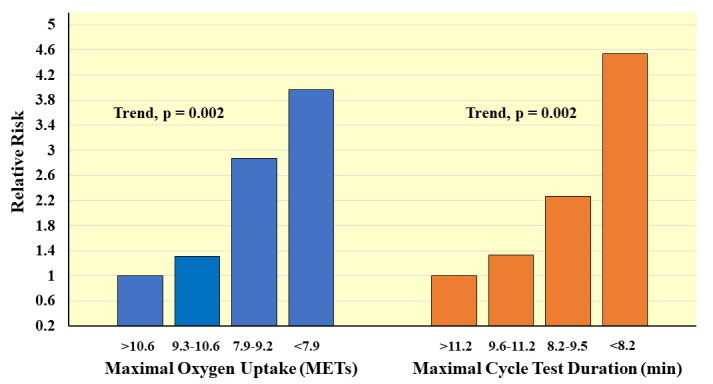
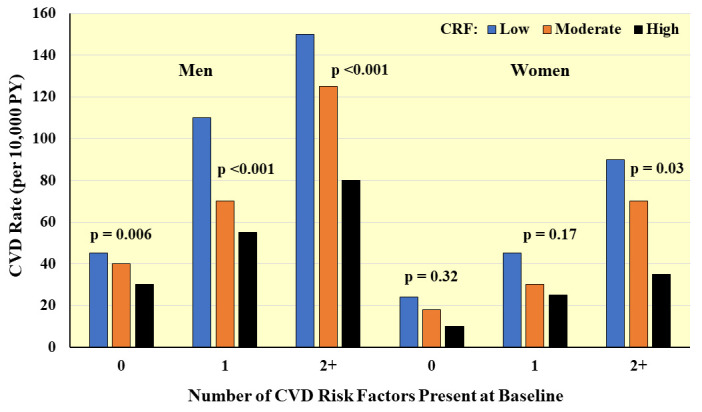
Cardiovascular disease (CVD) is the leading cause of death among adults in the U.S. and elsewhere. Variation in the presence, severity, and control of major modifiable risk factors accounts for much of the variation in CVD rates worldwide. Cardiorespiratory fitness (CRF) reflects the integration of ventilation, circulation, and metabolism for the delivery and utilization of oxygen in support of dynamic aerobic physical activity. The gold standard measure of CRF is maximal oxygen uptake. Because the primary factor underlying differences in this measure between individuals is maximal cardiac output, it can serve as a clinical indicator of cardiac function. Higher CRF is associated with favorable levels of major CVD risk factors, lower prevalence and severity of subclinical atherosclerosis, and lower risks of developing both primary and secondary clinical CVD events. The beneficial associations between CRF and CVD are seen in women and men, older and younger adults, in those with multiple coexisting risk factors or prior diagnosis of CVD. Exercise training and regular physical activity of at least moderate intensities and volumes improves CRF in adults, and improvements in CRF are associated with lower risks of subsequent CVD and mortality. Routine assessment of CRF in primary care settings could enhance individual-level CVD risk assessment and thereby guide implementation of appropriate measures to prevent future clinical events.
Keywords: exercise; exercise prescription; heart disease; maximal oxygen uptake; physical activity; prognosis; risk assessment.
Copyright: © 2022 The Author(s). Published by IMR Press.
Conflict of interest statement
The author declares no conflict of interest.
Figures
Similar articles
-
Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis.JAMA. 2009 May 20;301(19):2024-35. doi: 10.1001/jama.2009.681. JAMA. 2009. PMID: 19454641
-
Longitudinal algorithms to estimate cardiorespiratory fitness: associations with nonfatal cardiovascular disease and disease-specific mortality.J Am Coll Cardiol. 2014 Jun 3;63(21):2289-96. doi: 10.1016/j.jacc.2014.03.008. Epub 2014 Apr 2. J Am Coll Cardiol. 2014. PMID: 24703924 Free PMC article.
-
Comparison of objectively measured and estimated cardiorespiratory fitness to predict all-cause and cardiovascular disease mortality in adults: A systematic review and meta-analysis of 42 studies representing 35 cohorts and 3.8 million observations.J Sport Health Sci. 2024 Sep 11;14:100986. doi: 10.1016/j.jshs.2024.100986. Online ahead of print. J Sport Health Sci. 2024. PMID: 39271056 Free PMC article. Review.
-
Survival of the Fittest: Impact of Cardiorespiratory Fitness on Outcomes in Men and Women with Cardiovascular Disease.Clin Ther. 2020 Mar;42(3):385-392. doi: 10.1016/j.clinthera.2020.01.014. Epub 2020 Feb 20. Clin Ther. 2020. PMID: 32088022 Review.
-
Maintaining or increasing cardiorespiratory fitness is associated with reduced hospital admission rate.Eur J Prev Cardiol. 2024 Mar 4;31(4):436-444. doi: 10.1093/eurjpc/zwad367. Eur J Prev Cardiol. 2024. PMID: 38019572
Cited by
-
The association of non-exercise estimated cardiorespiratory fitness with hypertension and all-cause mortality in American and Chinese populations: evidence from NHANES and CHARLS.Front Cardiovasc Med. 2025 Apr 15;12:1497292. doi: 10.3389/fcvm.2025.1497292. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40303616 Free PMC article.
-
Associations Between Risk Factors of Cardiovascular Disease in Young Adults.Am J Lifestyle Med. 2024 Feb 20:15598276241233253. doi: 10.1177/15598276241233253. Online ahead of print. Am J Lifestyle Med. 2024. PMID: 39554940 Free PMC article.
-
The 100-Days: Physical Exercise and Challenges to Assess, Maintain and Improve Physical Fitness During Lockdown.Sports (Basel). 2024 Dec 5;12(12):337. doi: 10.3390/sports12120337. Sports (Basel). 2024. PMID: 39728877 Free PMC article.
-
The evolving role of cardiopulmonary exercise testing in ischemic heart disease - state of the art review.Curr Opin Cardiol. 2023 Nov 1;38(6):552-572. doi: 10.1097/HCO.0000000000001086. Epub 2023 Sep 21. Curr Opin Cardiol. 2023. PMID: 37610375 Free PMC article. Review.
-
The Impact of Body Composition on Cardiorespiratory Fitness in Adult Females.Cureus. 2024 Mar 3;16(3):e55428. doi: 10.7759/cureus.55428. eCollection 2024 Mar. Cureus. 2024. PMID: 38567237 Free PMC article.
References
-
- U.S. Department of Health and Human Services . Physical activity and health: A report of the Surgeon General . U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion; Atlanta, GA: 1996.
-
- Physical Activity Guidelines Advisory Committee . Physical Activity Guidelines Advisory Committee Report, 2008 . U.S. Department of Health and Human Services; Washington, DC: 2008. - PubMed
-
- Physical Activity Guidelines Advisory Committee . 2018 Physical Activity Guidelines Advisory Committee Scientific Report . U.S. Department of Health and Human Services; Washington, DC: 2018.
-
- Fletcher GF, Ades PA, Kligfield P, Arena R, Balady GJ, Bittner VA, et al. Exercise Standards for Testing and Training: a scientific statement from the American Heart Association. Circulation . 2013;128:873–934. - PubMed
-
- Ross R, Blair SN, Arena R, Church TS, Després J, Franklin BA, et al. Importance of Assessing Cardiorespiratory Fitness in Clinical Practice: a Case for Fitness as a Clinical Vital Sign: a Scientific Statement from the American Heart Association. Circulation . 2016;134:e653–e699. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
