

Atrioventricular Ring Tachycardias: Atypical Fast-Slow Atrioventricular Nodal Reentrant Tachycardia and Atrial Tachycardia Share a Common Arrhythmogenic Substrate-A Unifying Proposal
- PMID: 39076194
- PMCID: PMC11269071
- DOI: 10.31083/j.rcm2311369
Atrioventricular Ring Tachycardias: Atypical Fast-Slow Atrioventricular Nodal Reentrant Tachycardia and Atrial Tachycardia Share a Common Arrhythmogenic Substrate-A Unifying Proposal
Abstract
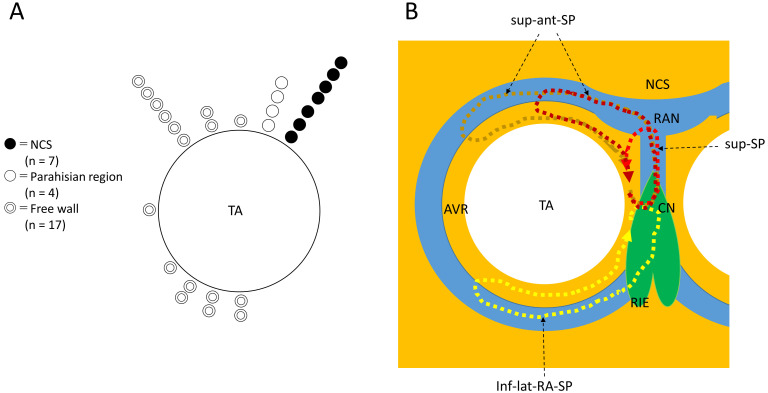
Our understanding of the variants of slow pathway (SP) and associated atypical atrioventricular (AV) nodal reentrant tachycardia (NRT) is still growing. We have identified variants extending outside Koch's triangle along the tricuspid annulus, including superior, superoanterior and inferolateral right atrial SP and associated atypical, fast-slow AVNRT. We review the history of each variant, their electrophysiological characteristics and related atypical AVNRT, and their treatment by catheter ablation. We focused our efforts on organizing the published information, as well as some unpublished, reliable data, and show the pitfalls of electrophysiological observations, along with keys to the diagnosis of atypical AVNRT. The superior-type of fast-slow AVNRT mimics adenosine-sensitive atrial tachycardia originating near the AV node and can be successfully treated by ablation of a superior SP form the right side of the perihisian region or from the non-coronary sinus of Valsalva. Fast-slow AVNRT using a superoanterior or inferolateral right atrial SP also mimics atrial tachycardia originating from the tricuspid annulus. We summarize the similarities among these variants of SP, and the origin of the atrial tachycardias, including their anatomical distributions and electrophysiological and pharmacological characteristics. Moreover, based on recent basic research reporting the presence of node-like AV ring tissue encircling the annuli in adult hearts, we propose the term "AV ring tachycardia" to designate the tachycardias that share the AV ring tissue as a common arrhythmogenic substrate. This review should help the readers recognize rare types of SP variants and associated AVNRT, and diagnose and cure these complex tachycardias. We hope, with this proposal of a unified tachycardia designation, to open a new chapter in clinical electrophysiology.
Keywords: adenosine sensitivity; atrial tachycardia; atrioventricular nodal reentrant tachycardia; atrioventricular ring; slow pathway; tricuspid annulus.
Copyright: © 2022 The Author(s). Published by IMR Press.
Conflict of interest statement
The authors declare no conflict of interest. Yoshiaki Kaneko is serving as one of the Guest editors of this journal. We declare that Yoshiaki Kaneko had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Giacomo Mugnai.
Figures
References
-
- Moe GK, Preston JB, Burlington H. Physiologic evidence for a dual A-V transmission system. Circulation Research . 1956;4:357–375. - PubMed
-
- Denes P, Wu D, Dhingra RC, Chuquimia R, Rosen KM. Demonstration of Dual A-V Nodal Pathways in Patients with Paroxysmal Supraventricular Tachycardia. Circulation . 1973;48:549–555. - PubMed
-
- Sung RJ, Styperek JL, Myerburg RJ, Castellanos A. Initiation of two distinct forms of atrioventricular nodal reentrant tachycardia during programmed ventricular stimulation in man. The American Journal of Cardiology . 1978;42:404–415. - PubMed
-
- Sung RJ, Waxman HL, Saksena S, Juma Z. Sequence of retrograde atrial activation in patients with dual atrioventricular nodal pathways. Circulation . 1981;64:1059–1067. - PubMed
-
- Ross DL, Johnson DC, Denniss AR, Cooper MJ, Richards DA, Uther JB. Curative surgery for atrioventricular junctional (“AV Nodal”) reentrant tachycardia. Journal of the American College of Cardiology . 1985;6:1383–1392. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
