

The Relationship between the Ratio of Urine Osmolality to Serum Osmolality and Neurological Outcomes in Out-of-hospital Cardiac Arrest Patients
- PMID: 39076503
- PMCID: PMC11267209
- DOI: 10.31083/j.rcm2505157
The Relationship between the Ratio of Urine Osmolality to Serum Osmolality and Neurological Outcomes in Out-of-hospital Cardiac Arrest Patients
Abstract
Background: Progressive ischemic brain injury after cardiac arrest can cause damage to the hypothalamic-pituitary axis, particularly the pituitary gland. This may impact serum osmolality (SOsm) and urine osmolality (UOsm) in patients who have experienced out-of-hospital cardiac arrest (OHCA). We assumed that a low ratio of UOsm to SOsm (USR) is related to poor outcomes among OHCA patients. Therefore, the present study was designed to evaluate the association between the USR within 72 h after the restoration of spontaneous circulation (ROSC) and 6-month neurological outcomes in OHCA patients.
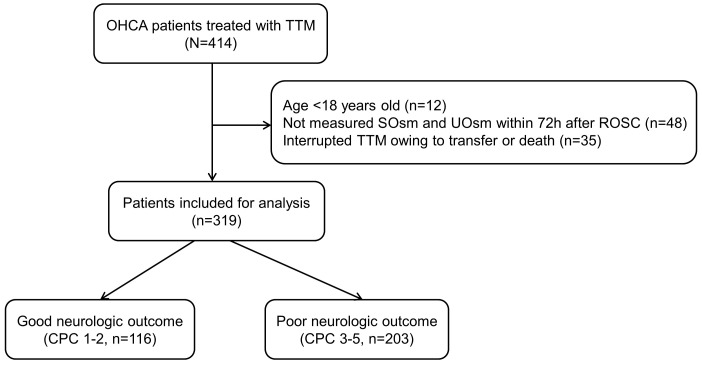
Methods: This prospective, observational study included OHCA patients with targeted temperature management at Chonnam National University Hospital in Gwangju, Korea, between January 2016 and December 2022. We collected SOsm and UOsm data at admission (T0) and 24 (T1), 48 (T2), and 72 h (T3) after ROSC. The primary outcome was a poor neurological outcome at 6 months defined by cerebral performance categories 3, 4, or 5.
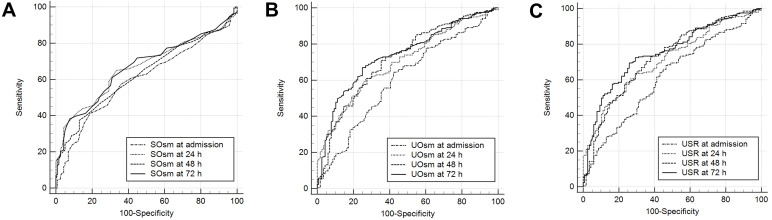
Results: This study included 319 patients. The mean UOsm and USRs at T0, T1, T2, and T3 of patients with poor outcomes were lower than those of patients with good outcomes. Multivariable analysis indicated that the USRs at T1 (odds ratio [OR], 0.363; 95% confidence interval [CI], 0.221-0.594), T2 (OR, 0.451; 95% CI, 0.268-0.761), and T3 (OR, 0.559; 95% CI, 0.357-0.875) were associated with a poor outcome. The areas under the receiver operating characteristic curves of USRs at T0, T1, T2, and T3 for predicting poor outcomes were 0.615 (95% CI, 0.559-0.669), 0.711 (95% CI, 0.658-0.760), 0.724 (95% CI, 0.671-0.772), and 0.751 (95% CI, 0.699-0.797), respectively.
Conclusions: The USRs within 72 h of ROSC were associated with poor neurological outcomes at 6 months in OHCA patients.
Keywords: cardiac arrest; prognosis; serum osmolality; targeted temperature management; urine osmolality.
Copyright: © 2024 The Author(s). Published by IMR Press.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Tsao CW, Aday AW, Almarzooq ZI, Alonso A, Beaton AZ, Bittencourt MS, et al. Heart Disease and Stroke Statistics-2022 Update: A Report From the American Heart Association. Circulation . 2022;145:e153–e639. - PubMed
-
- Chae MK, Lee JH, Lee TR, Yoon H, Hwang SY, Cha WC, et al. Early central diabetes insipidus: An ominous sign in post-cardiac arrest patients. Journal of Critical Care . 2016;32:63–67. - PubMed
-
- Lee DH, Lee BK, Song KH, Jung YH, Park JS, Lee SM, et al. Prevalence and risk factors for central diabetes insipidus in cardiac arrest survivor treated with targeted temperature management. The American Journal of Emergency Medicine . 2016;34:1400–1405. - PubMed
LinkOut - more resources
Full Text Sources
