

Electroencephalography Monitoring for Preventing Postoperative Delirium and Postoperative Cognitive Decline in Patients Undergoing Cardiothoracic Surgery: A Meta-Analysis
- PMID: 39076572
- PMCID: PMC11264044
- DOI: 10.31083/j.rcm2504126
Electroencephalography Monitoring for Preventing Postoperative Delirium and Postoperative Cognitive Decline in Patients Undergoing Cardiothoracic Surgery: A Meta-Analysis
Abstract
Background: Patients undergoing cardiothoracic surgery frequently encounter perioperative neurocognitive disorders (PND), which can include postoperative delirium (POD) and postoperative cognitive decline (POCD). Currently, there is not enough evidence to support the use of electroencephalograms (EEGs) in preventing POD and POCD among cardiothoracic surgery patients. This meta-analysis examined the importance of EEG monitoring in POD and POCD.
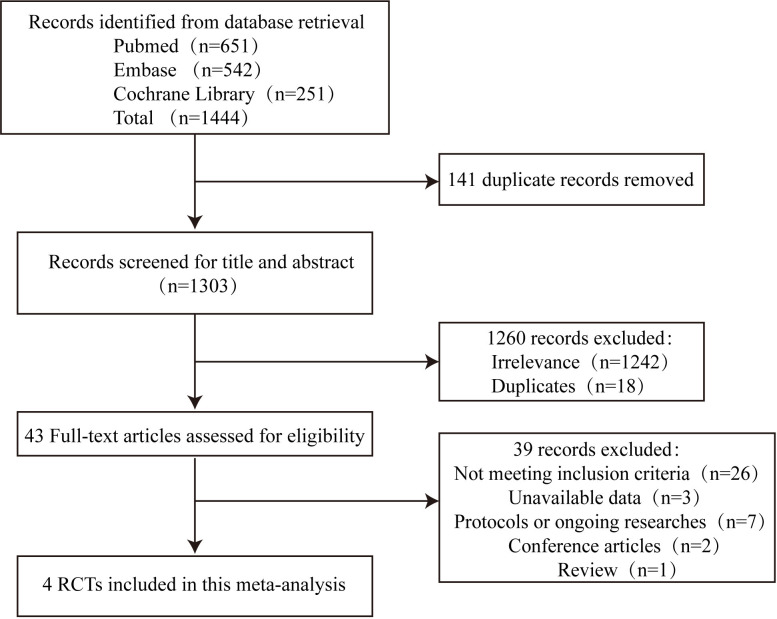
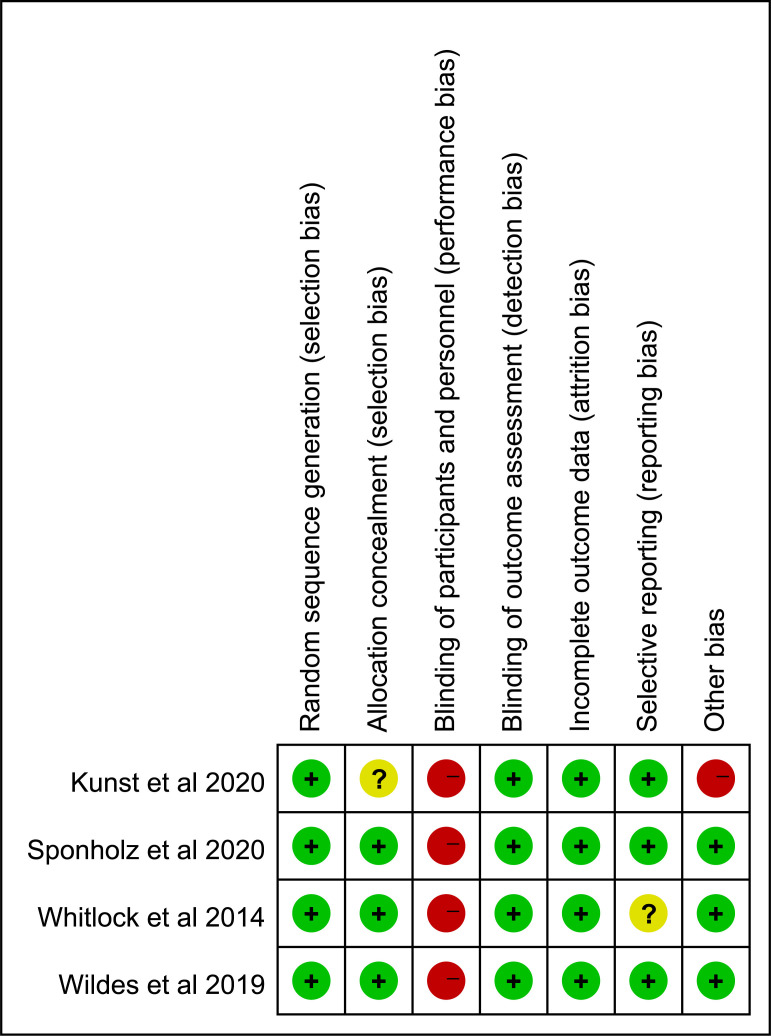
Methods: Cochrane Library, PubMed, and EMBASE databases were searched to obtain the relevant literature. This analysis identified trials based on the inclusion and exclusion criteria. The Cochrane tool was used to evaluate the methodological quality of the included studies. Review Manager software (version 5.3) was applied to analyze the data.
Results: Four randomized controlled trials (RCTs) were included in this meta-analysis, with 1096 participants. Our results found no correlation between EEG monitoring and lower POD risk (relative risk (RR): 0.81; 95% CI: 0.55-1.18; p = 0.270). There was also no statistically significant difference between the EEG group and the control group in the red cell transfusions (RR: 0.86; 95% CI: 0.51-1.46; p = 0.590), intensive care unit (ICU) stay (mean deviation (MD): -0.46; 95% CI: -1.53-0.62; p = 0.410), hospital stay (MD: -0.27; 95% CI: -2.00-1.47; p = 0.760), and mortality (RR: 0.33; 95% CI: 0.03-3.59; p = 0.360). Only one trial reported an incidence of POCD, meaning we did not conduct data analysis on POCD risk.
Conclusions: This meta-analysis did not find evidence supporting EEG monitoring as a potential method to reduce POD incidence in cardiothoracic surgery patients. In the future, more high-quality RCTs with larger sample sizes are needed to validate the relationship between EEG monitoring and POD/POCD further.
Keywords: cardiothoracic surgery; cognition disorders; cognitive dysfunction; delirium; electroencephalography monitoring; postoperative cognitive complications; postoperative cognitive decline; postoperative delirium.
Copyright: © 2024 The Author(s). Published by IMR Press.
Conflict of interest statement
The authors declare no conflict of interest. Hong Liu is serving as Guest Editor of this journal. We declare that Hong Liu had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Sophie Mavrogeni.
Figures




References
-
- Evered L, Scott DA, Silbert B, Maruff P. Postoperative cognitive dysfunction is independent of type of surgery and anesthetic. Anesthesia and Analgesia . 2011;112:1179–1185. - PubMed
-
- Robinson TN, Raeburn CD, Tran ZV, Angles EM, Brenner LA, Moss M. Postoperative delirium in the elderly: risk factors and outcomes. Annals of Surgery . 2009;249:173–178. - PubMed
-
- Bekker AY, Weeks EJ. Cognitive function after anaesthesia in the elderly. Best Practice & Research. Clinical Anaesthesiology . 2003;17:259–272. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
