

Athlete's Heart: A Cardiovascular Step-By-Step Multimodality Approach
- PMID: 39076743
- PMCID: PMC11273059
- DOI: 10.31083/j.rcm2405151
Athlete's Heart: A Cardiovascular Step-By-Step Multimodality Approach
Abstract
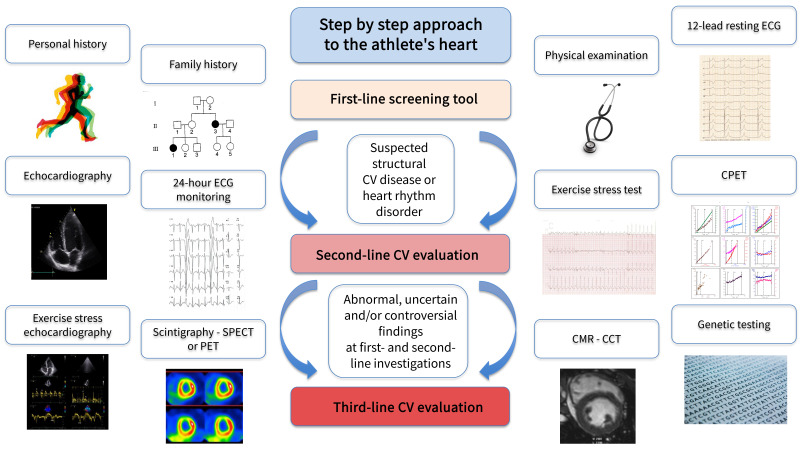
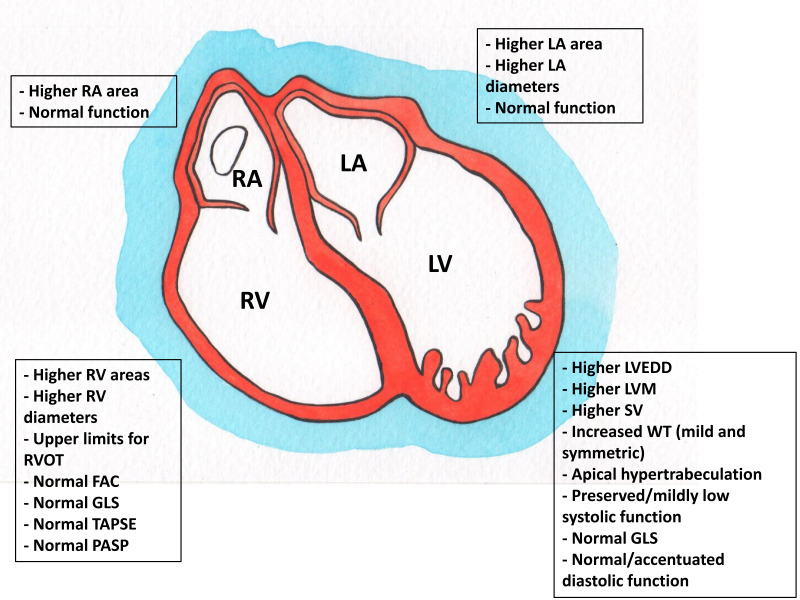
"Athlete's heart" is a spectrum of morphological, functional, and regulatory changes that occur in people who practice regular and long-term intense physical activity. The morphological characteristics of the athlete's heart may overlap with some structural and electrical cardiac diseases that may predispose to sudden cardiac death, including inherited and acquired cardiomyopathies, aortopathies and channelopathies. Overdiagnosis should be avoided, while an early identification of underlying cardiac life-threatening disorders is essential to reduce the potential for sudden cardiac death. A step-by-step multimodality approach, including a first-line evaluation with personal and family history, clinical evaluation, 12-lead resting electrocardiography (ECG), followed by second and third-line investigations, as appropriate, including exercise testing, resting and exercise echocardiography, 24-hour ECG Holter monitoring, cardiac magnetic resonance, computed tomography, nuclear scintigraphy, or genetic testing, can be determinant to differentiate between extreme physiology adaptations and cardiac pathology. In this context, cardiovascular imaging plays a key role in detecting structural abnormalities in athletes who fall into the grey zone between physiological adaptations and a covert or early phenotype of cardiovascular disease.
Keywords: athlete's heart; cardiovascular imaging; pre-participation screening; sports activity; sports cardiology; sudden cardiac death.
Copyright: © 2023 The Author(s). Published by IMR Press.
Conflict of interest statement
The authors declare no conflict of interest. Elena Cavarretta is serving as one of the Guest editors and Giuseppe Limongelli is serving as one of the Editorial Board members of this journal. We declare that Elena Cavarretta and Giuseppe Limongelli had no involvement in the peer review of this article and have no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Zhonghua Sun.
Figures
References
-
- Maron BJ, Levine BD, Washington RL, Baggish AL, Kovacs RJ, Maron MS, et al. Eligibility and Disqualification Recommendations for Competitive Athletes With Cardiovascular Abnormalities: Task Force 2: Preparticipation Screening for Cardiovascular Disease in Competitive Athletes: A Scientific Statement From the American Heart Association and American College of Cardiology. Circulation . 2015;132:e267–e272. - PubMed
-
- De Innocentiis C, Ricci F, Khanji MY, Aung N, Tana C, Verrengia E, et al. Athlete’s Heart: Diagnostic Challenges and Future Perspectives. Sports Medicine . 2018;48:2463–2477. - PubMed
-
- Prior DL, La Gerche A. The athlete’s heart. Heart . 2012;98:947–955. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
