

Characteristics of Pediatric In-Hospital Cardiac Arrests and Resuscitation Duration
- PMID: 39078626
- PMCID: PMC11289702
- DOI: 10.1001/jamanetworkopen.2024.24670
Characteristics of Pediatric In-Hospital Cardiac Arrests and Resuscitation Duration
Erratum in
-
Error in Abstract.JAMA Netw Open. 2024 Aug 1;7(8):e2435956. doi: 10.1001/jamanetworkopen.2024.35956. JAMA Netw Open. 2024. PMID: 39196566 Free PMC article. No abstract available.
Abstract
Importance: Cardiopulmonary resuscitation (CPR) duration is associated with cardiac arrest survival.
Objectives: To describe characteristics associated with CPR duration among hospitalized children without return of circulation (ROC) (patient-level analysis) and determine whether hospital median CPR duration in patients without ROC is associated with survival (hospital-level analysis).
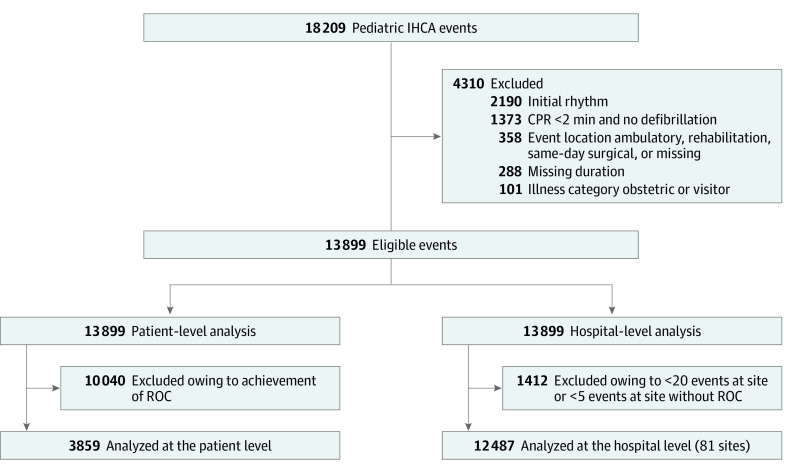
Design, setting, and participants: This retrospective cohort study of patients undergoing pediatric in-hospital CPR between January 1, 2000, and December 31, 2021, used data from the Get With the Guidelines-Resuscitation registry. Children receiving chest compressions for at least 2 minutes and/or defibrillation were included in the patient-level analysis. For the hospital-level analysis, sites with at least 20 total events and at least 5 events without ROC were included. Data were analyzed from December 1, 2022, to November 15, 2023.
Exposures: For the patient-level analysis, the exposure was CPR duration in patients without ROC. For the hospital-level analysis, the exposure was quartile of median CPR duration in events without ROC at each hospital.
Main outcomes and measures: For the patient-level analysis, outcomes were patient and event factors, including race and ethnicity and event location; we used a multivariable hierarchical linear regression model to assess factors associated with CPR duration in patients without ROC. For the hospital-level analysis, the main outcome was survival to discharge among all site events; we used a random intercept multivariable hierarchical logistic regression model to examine the association between hospital quartile of CPR duration and survival to discharge.
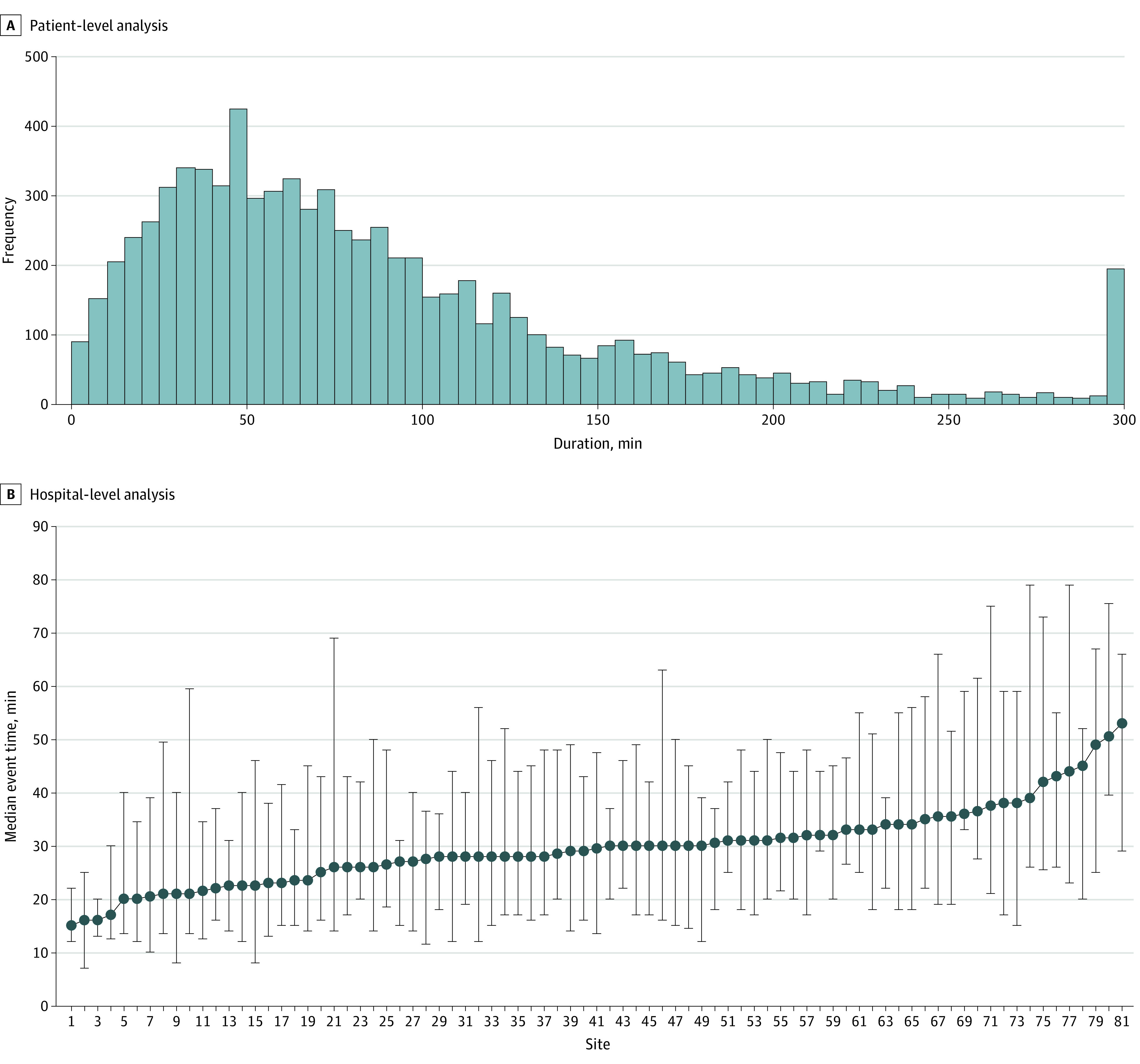
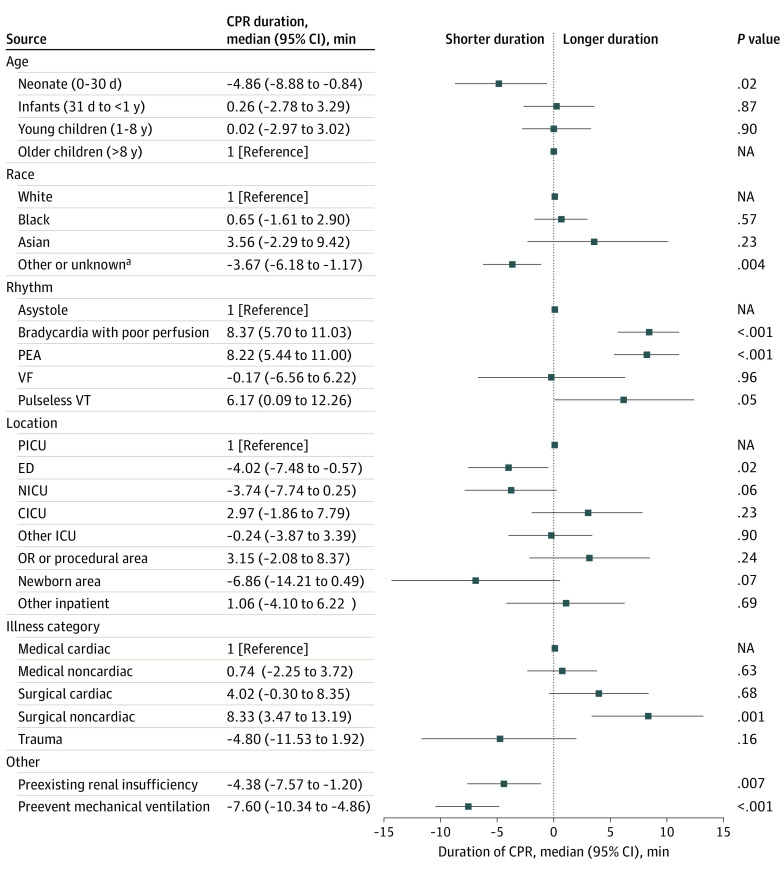
Results: Of 13 899 events, 3859 patients did not have ROC (median age, 7 months [IQR, 0 months to 7 years]; 2175 boys [56%]). Among event nonsurvivors, median CPR duration was longer in those with initial rhythms of bradycardia with poor perfusion (8.37 [95% CI, 5.70-11.03] minutes; P < .001), pulseless electrical activity (8.22 [95% CI, 5.44-11.00] minutes; P < .001), and pulseless ventricular tachycardia (6.17 [95% CI, 0.09-12.26] minutes; P = .047) (vs asystole). Shorter median CPR duration was associated with neonates compared with older children (-4.86 [95% CI, -8.88 to -0.84] minutes; P = .02), emergency department compared with pediatric intensive car7 e unit location (-4.02 [95% CI, -7.48 to -0.57] minutes; P = .02), and members of racial or ethnic minority groups compared with White patients (-3.67 [95% CI, -6.18 to -1.17]; P = .004). Among all CPR events, the adjusted odds of survival to discharge differed based on hospital quartile of median CPR duration among events without ROC; compared with quartile 1 (15.0-25.9 minutes), the adjusted odds ratio for quartile 2 (26.0-29.4 minutes) was 1.22 (95% CI, 1.09-1.36; P < .001); for quartile 3 (29.5-32.9 minutes), 1.23 (95% CI, 1.08-1.39; P = .002); and for quartile 4 (33.0-53.0 minutes), 1.04 (95% CI, 0.91-1.19; P = .58).
Conclusions and relevance: In this retrospective cohort study of pediatric in-hospital CPR, several factors, including age and event location, were associated with CPR duration in event nonsurvivors. The odds of survival to discharge were lower for patients at hospitals with the shortest and longest median CPR durations among events without ROC. Further studies are needed to determine the optimal duration of CPR during pediatric in-hospital cardiac arrest and to provide training guidelines for resuscitation teams to eliminate disparities in resuscitation care.
Conflict of interest statement
Figures
References
-
- Holmberg MJ, Ross CE, Fitzmaurice GM, et al. ; American Heart Association’s Get With The Guidelines–Resuscitation Investigators . Annual incidence of adult and pediatric in-hospital cardiac arrest in the United States. Circ Cardiovasc Qual Outcomes. 2019;12(7):e005580. doi: 10.1161/CIRCOUTCOMES.119.005580 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
