

Effect of automated versus conventional ventilation on mechanical power of ventilation-A randomized crossover clinical trial
- PMID: 39078857
- PMCID: PMC11288413
- DOI: 10.1371/journal.pone.0307155
Effect of automated versus conventional ventilation on mechanical power of ventilation-A randomized crossover clinical trial
Abstract
Introduction: Mechanical power of ventilation, a summary parameter reflecting the energy transferred from the ventilator to the respiratory system, has associations with outcomes. INTELLiVENT-Adaptive Support Ventilation is an automated ventilation mode that changes ventilator settings according to algorithms that target a low work-and force of breathing. The study aims to compare mechanical power between automated ventilation by means of INTELLiVENT-Adaptive Support Ventilation and conventional ventilation in critically ill patients.
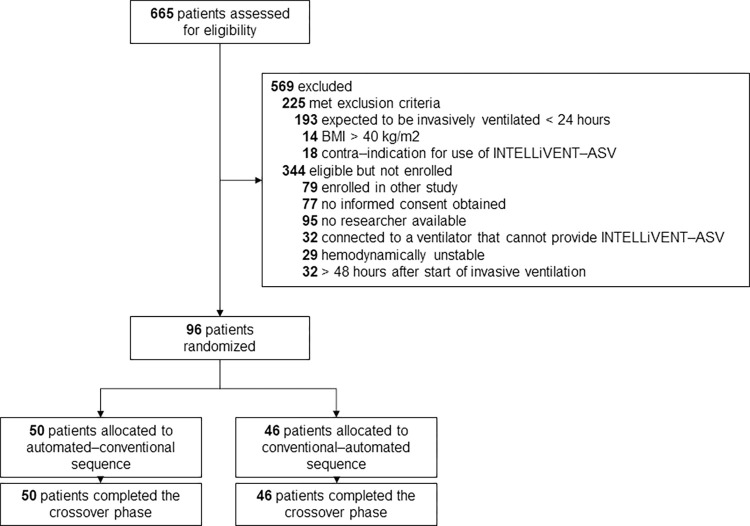
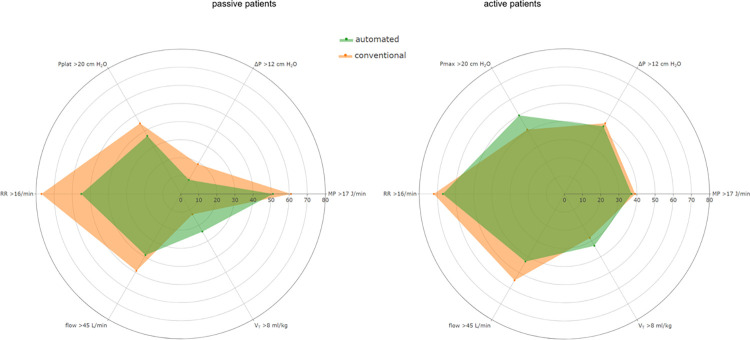
Materials and methods: International, multicenter, randomized crossover clinical trial in patients that were expected to need invasive ventilation > 24 hours. Patients were randomly assigned to start with a 3-hour period of automated ventilation or conventional ventilation after which the alternate ventilation mode was selected. The primary outcome was mechanical power in passive and active patients; secondary outcomes included key ventilator settings and ventilatory parameters that affect mechanical power.
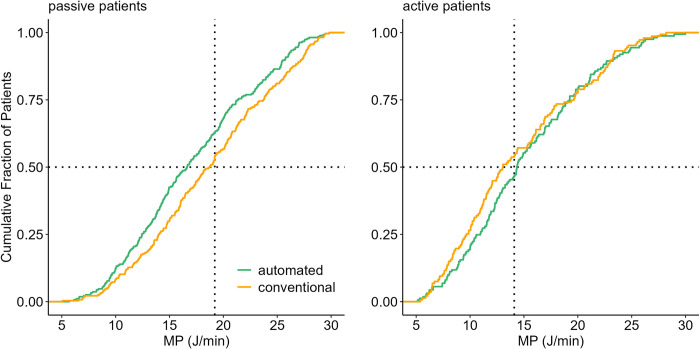
Results: A total of 96 patients were randomized. Median mechanical power was not different between automated and conventional ventilation (15.8 [11.5-21.0] versus 16.1 [10.9-22.6] J/min; mean difference -0.44 (95%-CI -1.17 to 0.29) J/min; P = 0.24). Subgroup analyses showed that mechanical power was lower with automated ventilation in passive patients, 16.9 [12.5-22.1] versus 19.0 [14.1-25.0] J/min; mean difference -1.76 (95%-CI -2.47 to -10.34J/min; P < 0.01), and not in active patients (14.6 [11.0-20.3] vs 14.1 [10.1-21.3] J/min; mean difference 0.81 (95%-CI -2.13 to 0.49) J/min; P = 0.23).
Conclusions: In this cohort of unselected critically ill invasively ventilated patients, automated ventilation by means of INTELLiVENT-Adaptive Support Ventilation did not reduce mechanical power. A reduction in mechanical power was only seen in passive patients.
Study registration: Clinicaltrials.gov (study identifier NCT04827927), April 1, 2021.
Url of trial registry record: https://clinicaltrials.gov/study/NCT04827927?term=intellipower&rank=1.
Copyright: © 2024 Buiteman-Kruizinga et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
LBK received fees from Hamilton Medical for lecturing. MJS was part-time employed as a team leader of Research and New Technologies at Hamilton Medical from January 2022 till January 2023. The other authors declare no conflicts of interest.
Figures
References
-
- Serpa Neto A, Amato MBP, Schultz MJ. Dissipated Energy is a Key Mediator of VILI: Rationale for Using Low Driving Pressures. In: Vincent J-L, editor. Annual Update in Intensive Care and Emergency Medicine 2016. Cham: Springer International Publishing; 2016. p. 311–21.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
