

Clinical utility of a rapid two-dimensional balanced steady-state free precession sequence with deep learning reconstruction
- PMID: 39079600
- PMCID: PMC11367510
- DOI: 10.1016/j.jocmr.2024.101069
Clinical utility of a rapid two-dimensional balanced steady-state free precession sequence with deep learning reconstruction
Abstract
Background: Cardiovascular magnetic resonance (CMR) cine imaging is still limited by long acquisition times. This study evaluated the clinical utility of an accelerated two-dimensional (2D) cine sequence with deep learning reconstruction (Sonic DL) to decrease acquisition time without compromising quantitative volumetry or image quality.
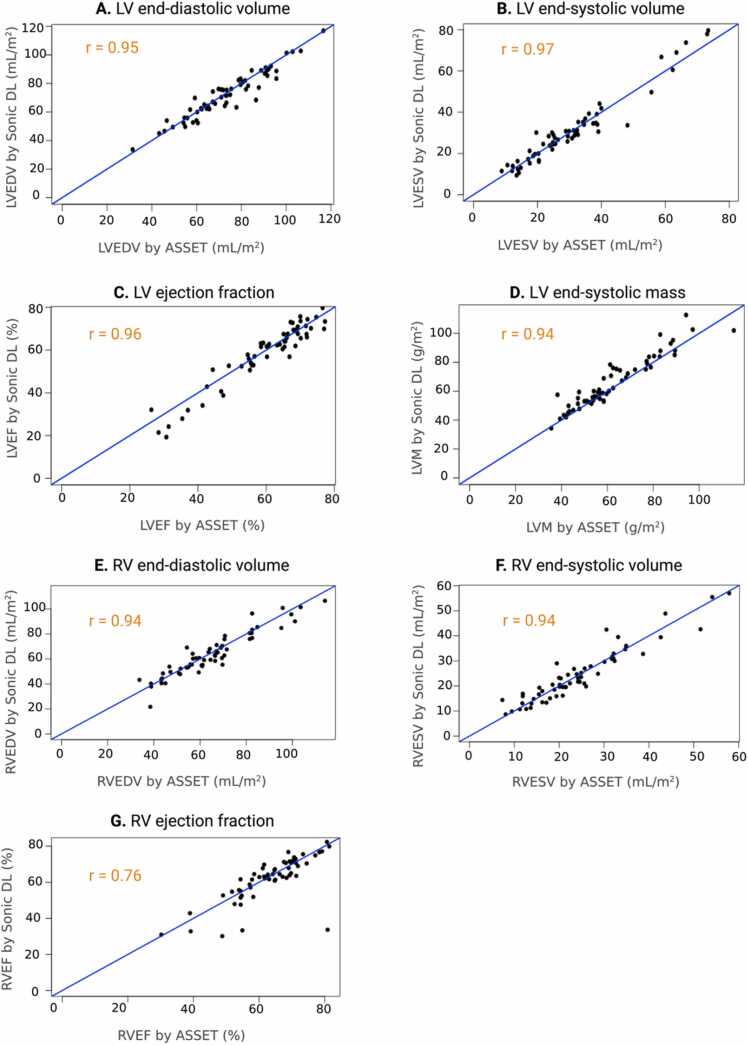
Methods: A sub-study using 16 participants was performed using Sonic DL at two different acceleration factors (8× and 12×). Quantitative left-ventricular volumetry, function, and mass measurements were compared between the two acceleration factors against a standard cine method. Following this sub-study, 108 participants were prospectively recruited and imaged using a standard cine method and the Sonic DL method with the acceleration factor that more closely matched the reference method. Two experienced clinical readers rated images based on their diagnostic utility and performed all image contouring. Quantitative contrast difference and endocardial border sharpness were also assessed. Left- and right-ventricular volumetry, left-ventricular mass, and myocardial strain measurements were compared between cine methods using Bland-Altman plots, Pearson's correlation, and paired t-tests. Comparative analysis of image quality was measured using Wilcoxon-signed-rank tests and visualized using bar graphs.
Results: Sonic DL at an acceleration factor of 8 more closely matched the reference cine method. There were no significant differences found across left ventricular volumetry, function, or mass measurements. In contrast, an acceleration factor of 12 resulted in a 6% (5.51/90.16) reduction of measured ejection fraction when compared to the standard cine method and a 4% (4.32/88.98) reduction of measured ejection fraction when compared to Sonic DL at an acceleration factor of 8. Thus, Sonic DL at an acceleration factor of 8 was chosen for downstream analysis. In the larger cohort, this accelerated cine sequence was successfully performed in all participants and significantly reduced the acquisition time of cine images compared to the standard 2D method (reduction of 37% (5.98/16) p < 0.0001). Diagnostic image quality ratings and quantitative image quality evaluations were statistically not different between the two methods (p > 0.05). Left- and right-ventricular volumetry and circumferential and radial strain were also similar between methods (p > 0.05) but left-ventricular mass and longitudinal strain were over-estimated using the proposed accelerated cine method (mass over-estimated by 3.36 g/m2, p < 0.0001; longitudinal strain over-estimated by 1.97%, p = 0.001).
Conclusion: This study found that an accelerated 2D cine method with DL reconstruction at an acceleration factor of 8 can reduce CMR cine acquisition time by 37% (5.98/16) without significantly affecting volumetry or image quality. Given the increase of scan time efficiency, this undersampled acquisition method using deep learning reconstruction should be considered for routine clinical CMR.
Keywords: Accelerated imaging; CMR; Cardiac function; Clinical utility; Deep learning reconstruction; Diagnostic accuracy.
Crown Copyright © 2024. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of competing interests The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Matthias Friedrich reports financial support was provided by MEDTEQ and GE Healthcare. Matthias Friedrich reports a relationship with Circle Cardiovascular Imaging Inc that includes board membership. Martin Janich, Junjie Ma, and Xucheng Zhu report a relationship with GE Healthcare that includes employment. The other authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures







References
-
- Grothues F., Smith G.C., Moon J.C.C., Bellenger N.G., Collins P., Klein H.U., et al. Comparison of interstudy reproducibility of cardiovascular magnetic resonance with two-dimensional echocardiography in normal subjects and in patients with heart failure or left ventricular hypertrophy. Am J Cardiol. 2002;90(1):29–34. https://www.sciencedirect.com/science/article/pii/S0002914902023810 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
